The Walnut-Sized Anchor: What Exactly Changes When the Prostate Vanishes?
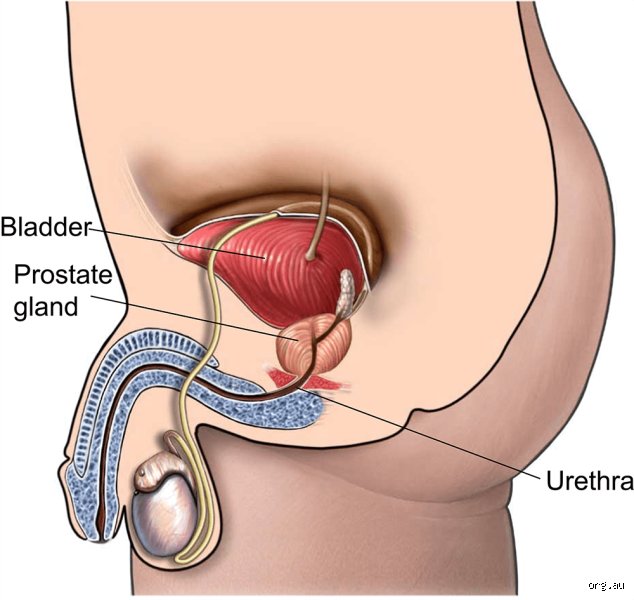
To understand the chaos that follows, we have to look at what was actually stolen by the scalpel. The prostate isn't just sitting there doing nothing; it is a walnut-sized gland wrapped around the urethra, nestled right below the bladder. Its primary gig is secreting the fluid that nourishes and transports sperm. But when a surgeon hacks it out—usually because of adenocarcinoma—they aren't just taking the gland.
Anatomical Collateral Damage in the Pelvic Floor
They are removing a literal junction box. Think about it as removing a central transit hub from a subway system while trying to keep the trains running. Because the urethra runs directly through the center of the prostate, the surgeon must slice the tube, pull the bladder down, and stitch the remaining urethra directly to the bladder neck. This new connection is called a vesicourethral anastomosis. But here is where it gets tricky: the nerves and blood vessels that control erections—the delicate cavernous nerves—run like a spiderweb right along the surface of the prostate. Even with the most meticulous robotic surgery at a world-class center like the Mayo Clinic, these fibers get stretched, bruised, or completely severed.
The Disruption of the Urinary Sphincter Complex
Then there is the plumbing problem. You have two urinary sphincters: an internal one at the bladder neck and an external one lower down. Surgery almost always obliterates the internal sphincter. Suddenly, the external sphincter—a ring of muscle that used to share the workload—is forced to do 100% of the heavy lifting. If that muscle isn't in Olympic-level shape, you leak. Plain and simple.
The Immediate Aftermath: Catheters, Clots, and the First Thirty Days
Nobody talks enough about the first month, yet that changes everything. You wake up from anesthesia in the recovery room, perhaps at Johns Hopkins or a local regional hospital, and the very first thing you notice is a silicone tube snaking out of your penis. That is the indwelling Foley catheter, and it will be your mandatory, highly annoying companion for the next 7 to 14 days.
The Mandatory Foley Catheter Era
Why is it there? It is not just to collect urine while you heal. Its main job is acting as a physical stent to hold that brand-new vesicourethral anastomosis open and stable while the tissues fuse back together. Without it, the scar tissue would contract, closing off the airway of your bladder entirely. I think we underestimate the psychological toll of walking around with a plastic bag of your own urine strapped to your calf. It is a stark, unglamorous introduction to the post-prostatectomy reality.
The Healing Curve and Early Complications
During these initial weeks, bladder spasms are common. The bladder is pissed off—literally. It has been yanked downward and stitched to a new spot. It reacts by cramping violently, forcing urine to leak around the sides of the catheter. Doctors routinely prescribe anticholinergic medications like oxybutynin to quiet the storm, but the physical discomfort is only part of the equation. There is also the constant vigilance for hematuria—blood clots in the urine that can block the catheter entirely—and the looming threat of deep vein thrombosis due to pelvic stagnation.
The Sexual Reconstruction: Dry Orgasms and the Erectile Landscape
Let us be brutally honest here because patients are often left in the dark by over-optimistic surgical brochures. If your prostate is gone, your seminal vesicles are gone too. This means you will never ejaculate fluid again. You can still have an orgasm—the neurological sensation remains intact because the pudendal nerve is untouched—but it will be a retrograde-style dry orgasm. It is a bizarre sensation that many men describe as feeling mechanically complete but visually surreal.
The Reality of Nerve-Sparing Surgery
Surgeons love to brag about "nerve-sparing" techniques, a concept pioneered by Dr. Patrick Walsh in 1982. But people don't think about this enough: "nerve-sparing" is a spectrum, not a guarantee. If the tumor is too close to the capsule, the surgeon must prioritize cancer clearance over sexual performance. Even if both nerve bundles are perfectly preserved, they go into a state of profound shock called neuropraxia. It takes anywhere from 12 to 24 months for these microscopic nerves to wake up. In the meantime, the lack of regular blood flow to the penis can cause cavernosal fibrosis, which leads to a permanent loss of penile length and elasticity. It is a use-it-or-lose-it scenario on a cellular level.
The Penile Rehabilitation Protocol
Which explains why modern urology clinics don't just wait around to see what happens. They initiate penile rehabilitation almost immediately after the catheter comes out. This involves forcing blood into the erectile tissue artificially. Patients are started on daily low-dose PDE5 inhibitors like Tadalafil, long before they even feel a spark of libido. If pills fail, the next step involves a vacuum erection device or even intracavernosal injections of Alprostadil directly into the shaft. It sounds terrifying, yet for many, it is the only way to prevent tissue atrophy while the nerves slowly rebuild their pathways.
Weighing the Alternatives: Did the Prostate Absolutely Have to Go?
The issue remains that radical surgery is a definitive, scorched-earth approach to prostate cancer. But we are far from the days when surgery was the only viable option for a localized tumor. Today, the medical community is deeply divided on whether every diagnosed man needs to rush to the operating theater.
Active Surveillance vs. Radical Intervention
For men with low-risk, localized disease—defined by a Gleason Score of 6 and a low PSA density—the modern gold standard is actually active surveillance. This isn't "watchful waiting," which is passive tracking for elderly patients; it is a rigorous protocol of serial PSA tests, multiparametric MRIs, and repeat biopsies. The goal is to delay or entirely avoid the side effects of surgery without sacrificing long-term survival. Experts disagree on the exact triggers for switching from surveillance to treatment, but the data shows that many men can safely live for decades with their prostates intact.
Radiation and Focal Therapies as Contenders
If treatment is mandatory, surgery isn't the only game in town. External beam radiation therapy combined with androgen deprivation, or brachytherapy—where radioactive seeds are implanted directly into the tissue—offer similar 10-year survival rates for many patient profiles. Furthermore, emerging focal therapies like High-Intensity Focused Ultrasound (HIFU) or cryotherapy seek to destroy only the tumor while leaving the rest of the healthy prostate intact. These alternatives significantly lower the rates of immediate impotence and incontinence, yet they carry their own risks, including radiation cystitis and the complication of salvage surgery if the cancer returns. It is a high-stakes chess match where every move has a cost.
Common mistakes and misconceptions
The myth of immediate, permanent impotence
Many patients assume that when a man's prostate is removed, his sex life vanishes instantly into thin air. That is simply wrong. While erectile dysfunction represents a formidable hurdle post-surgery, nerve-sparing techniques have revolutionized outcomes. Surgeons carefully peel the delicate cavernous nerves away from the prostate capsule. Your erections do not just disappear forever, though they do go into a state of shock. Regeneration takes time, often between 12 to 24 months. Let's be clear: the organ is gone, but the biological machinery for pleasure remains largely intact.
The confusion between semen and orgasm
Can you still climax without this specific gland? Absolutely. A widespread misunderstanding conflates fluid emission with the actual sensation of climax. Because the seminal vesicles and prostate are excised, a man will experience a dry orgasm. The pelvic muscles still contract rhythmically. The euphoric sensation in the brain remains identical. The issue remains that patients equate a lack of ejaculate with a lack of pleasure, which causes immense psychological anxiety that can actually inhibit recovery. It is a mental barrier, not a structural veto.
Believing incontinence is a lifelong sentence
Total, permanent urinary leakage is actually quite rare, affecting fewer than 5% of patients long-term. Yet, the fear of diapers dominates pre-operative discussions. Immediately after the urinary catheter is pulled out, leaking is common. The external urethral sphincter must learn to do all the heavy lifting alone. Physical therapy accelerates this retraining. Do not mistake a temporary three-month nuisance for a permanent lifestyle modification.
The overlooked impact of pelvic angle shifting
Structural changes in the lower pelvis
Everyone talks about nerves and leaking, but what about the literal void left behind in your lower abdomen? The prostate is roughly the size of a ping-pong ball, sitting right at the crossroads of your urinary tract. When it vanishes, the bladder drops slightly to close the gap. The surgeon pulls the bladder neck down to anastomose it directly to the remaining urethra. This structural displacement alters the anatomical angle of your pelvic floor. Have you ever considered how a minor shift in internal geometry alters your biomechanics? It changes how you experience abdominal pressure during sudden movements like coughing or lifting heavy weights. Except that nobody warns patients about this strange, hollow sensation during the initial healing phase (which feels distinct from muscle pain). This spatial realignment requires conscious core engagement, making targeted pelvic floor rehabilitation an absolute necessity rather than an optional chore.
Frequently Asked Questions
What happens to a man's testosterone levels after the prostate is removed?
The surgical excision of this gland does not affect your systemic hormone production. Because testosterone is synthesized inside the testicles, a radical prostatectomy leaves your primary masculinity engine untouched. Data from clinical registries show that serum testosterone levels remain stable post-operatively, fluctuating by less than 3% on average. Patients do not experience surgical menopause or sudden hot flashes from the removal itself. However, if your treatment protocol includes concurrent androgen deprivation therapy, that specific medication will plummet your hormone count, not the scalpel.
How long does it take for urinary control to return to normal?
Recovery follows a nonlinear trajectory that demands immense patience. Statistics indicate that approximately 60% of men achieve satisfactory continence within three months, a figure that climbs to roughly 88% by the one-year mark. Age, pre-existing sphincter strength, and the precise surgical approach dictate your personal timeline. Utilizing specialized biofeedback exercises can compress this recovery window significantly. As a result: dedication to your daily rehabilitation regimen directly influences how fast you discard those protective pads.
Can a man still father biological children after this operation?
Natural conception becomes impossible once the prostate gland and seminal vesicles are extracted. Since the anatomical highway connecting the testicles to the urethra is permanently severed, no fluid can transport the spermatozoa out of the body during intercourse. However, the testicles continue to manufacture viable sperm cells at a normal rate. Men who still wish to pursue fatherhood must utilize assistive reproductive technologies, such as testicular sperm extraction combined with in vitro fertilization. This requires proactive planning and sperm banking prior to entering the operating theatre.
A definitive perspective on post-surgical reality
We need to stop viewing radical prostatectomy as a form of anatomical castration. It is an aggressive, life-saving oncology intervention that undeniably alters intimacy and urination. Yet, the human body exhibits astonishing resilience when adapting to structural subtractions. Total recovery is not a passive waiting game; it requires aggressive physical rehabilitation and psychological fortitude. The problem is that medical literature often sterilizes the human experience into cold recovery percentages. Let's be clear: your masculinity is not localized within a single piece of pelvic tissue. Embracing the post-operative reality means redefining your relationship with your body, which explains why men who actively engage in rehabilitation report high quality-of-life scores within two years. In short, life changes dramatically, but it certainly does not end.