The Reality of the Clock: Why Time in the Operating Room Fluctuates So Wildly
People don't think about this enough, but when a surgeon quotes you a time frame, they are giving you the best-case scenario. The thing is, the prostate sits in a notoriously crowded anatomical neighborhood, wedged tightly between the bladder and the rectum, wrapped in a delicate web of nerves responsible for your future erectile function and urinary continence. That changes everything. A standard laparoscopic removal might wrap up in 150 minutes at a high-volume center like the Cleveland Clinic, yet a complex open surgery on a patient with a high body mass index could easily push past the four-hour mark. We are far from a one-size-fits-all timeline here.
The Definition of Surgical Time vs. Total Hospital Time
Where it gets tricky is differentiating between actual skin-to-skin operative time and the hours your family spends pacing the waiting room. The surgical clock only ticks while the surgeon is actively working. Yet, you must factor in an extra 60 to 90 minutes for pre-operative prep, endotracheal intubation, and positioning. And what about the immediate aftermath? The recovery room stay adds another two hours minimum as the anesthesia wears off. It is an exhausting marathon, frankly.
Anatomical Surprises That Can Stall the Surgeon
No two pelvises look identical on the inside. Because scar tissue from a forgotten childhood hernia repair or localized inflammation from chronic prostatitis can turn a straightforward dissection into a meticulous, millimeter-by-millimeter slog, the clock often stretches. Have you ever tried untangling headphones in the dark? That is what separating a tumor-ridden prostate from the neurovascular bundle feels like when visibility gets compromised by unexpected bleeding. Anatomy always dictates the tempo, not the hospital schedule.
Deconstructing the Techniques: How the Surgical Method Alters the Timeline
The specific method your urologist deploys is the heaviest lever pulling on the clock. Back in 2005, the vast majority of these interventions were open procedures requiring large incisions and manual retraction. Today, the landscape is dominated by technology, yet the shift toward innovation hasn't necessarily made the procedures faster—just different. Robotic-assisted laparoscopic radical prostatectomy (RALP) has become the gold standard, but it introduces its own unique temporal demands that families rarely anticipate before checking into the hospital.
The Robotic Approach: Efficiency Linked with Setup Time
If you opt for a da Vinci robotic system, the actual cutting and suturing might only take two to three hours in the hands of an expert. But the docking of the robot—aligning those massive mechanical arms with the trocars inserted into your abdomen—is a precise choreography that adds a mandatory 30 minutes to the room time. Yet, the precision it grants is undeniable. The high-definition 3D camera allows for an incredibly meticulous vesicourethral anastomosis, which is the fancy term for sewing the bladder back to the urethra after the prostate is gone. This structural reconstruction is the most critical phase of the entire event.
The Traditional Open Radical Prostatectomy: Old School and Fast?
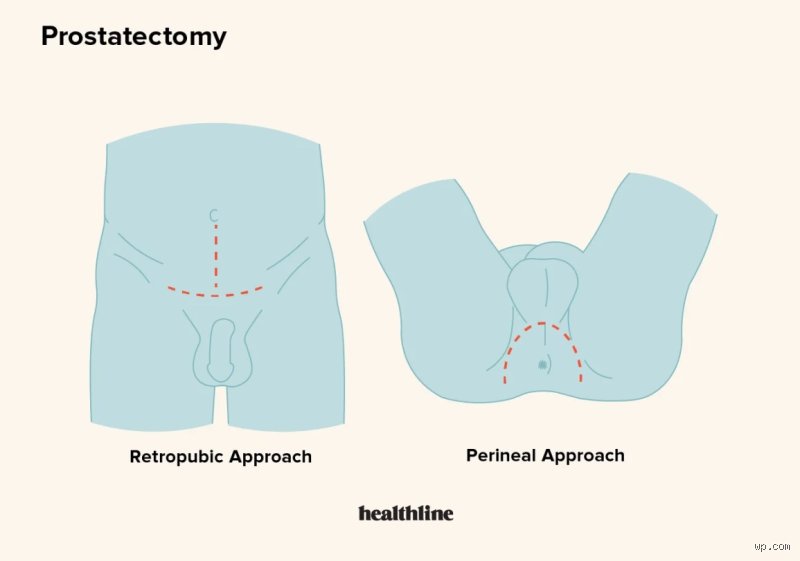
But wait, isn't the old-fashioned way quicker? Sometimes, yes. An experienced surgeon performing a retropubic open prostatectomy can occasionally finish in under 90 minutes because they do not have to contend with digital interfaces or gas insufflation to puff up the abdomen. Except that this speed comes at a cost. The blood loss is statistically higher, which explains why surgeons must move with deliberate caution, often slowing down to achieve meticulous hemostasis. It is a paradox: the older method can be faster on paper, but the physiological toll on your body is significantly more demanding.
The Invisible Time Add-Ons: Lymph Node Dissections and Staging
When calculating how many hours is prostate surgery, you cannot just look at the prostate itself. If your preoperative PSA levels or your Gleason score from the biopsy suggest a higher risk of metastasis, the surgeon cannot just grab the primary gland and leave. They have to hunt for hidden cancer cells. This means entering the pelvic sidewalls to perform a pelvic lymph node dissection (PLND), a secondary procedure that happens concurrently but wreaks havoc on the clock.
Standard vs. Extended Lymphadenectomy
A standard sampling of the obturator nodes might only tack on an extra 20 to 30 minutes to the overall operating time. However, if your medical team decides an extended lymph node dissection is required—mapping out the external iliac and hypogastric regions—the clock will aggressively leap forward by at least an hour or more. Honestly, it's unclear exactly how many nodes need to be removed for the perfect balance of survival benefit versus side effects; experts disagree fiercely on this point. I believe that a more aggressive dissection is usually worth the extra time on the table if it ensures cleaner margins, though it undeniably increases the risk of postoperative lymphedema.
Comparing Timelines: How Radical Removal Stacks Up Against Focal Alternatives
It helps to contextualize the length of a radical prostatectomy by looking at what else is on the medical menu. Not everyone needs the entire organ ripped out. If you are dealing with localized, low-intermediate risk disease, the time you spend under general anesthesia can be slashed dramatically by looking at ablative therapies rather than major extirpative surgery.
High-Intensity Focused Ultrasound (HIFU) and Cryotherapy
Consider High-Intensity Focused Ultrasound (HIFU), a technique where acoustic energy cooks the cancer cells transrectally. The whole thing is wrapped up in about 90 to 120 minutes, and because there are no incisions, the immediate recovery curve is entirely different. As a result: you are often out of the facility the very same afternoon. Cryotherapy, which freezes the tissue using argon gas needles guided by real-time ultrasound, follows a similar, abbreviated trajectory. But the issue remains that these focal treatments leave the rest of the prostate intact, meaning your long-term surveillance schedule will be far more intense than if you had undergone the full three-hour radical surgery to begin with.
Common misconceptions about surgical timing
The faster, the better myth
Speed is a terrible metric for surgical excellence. Patients often grill their urologists about the ticking clock, convinced that a ninety-minute procedure beats a three-hour marathon. The problem is that rushing breeds complications. A surgeon racing against an arbitrary stopwatch might compromise the meticulous sparing of the cavernous nerves, which explains why a slightly longer, deliberate operation often yields far superior long-term potency outcomes. Let's be clear: deliberate precision trumps rapid execution every single time you are on the operating table.
Technology guarantees a shortcut
Everyone assumes the da Vinci robot operates with lightning speed. Except that docking the robotic arms, calibrating the 3D high-definition optics, and positioning the patient takes significant time before the first incision is even deepened. A novice surgeon using state-of-the-art robotics might require four hours, yet an experienced open surgeon could finish in ninety minutes. How many hours is prostate surgery? It depends vastly on the human driving the machine, not just the hardware itself. The mechanical arms are merely extensions of human fingers, which means robotic efficiency requires immense surgeon expertise to actually translate into reduced anesthesia time.
The hidden variable: Pelvic anatomy complications
Hostile pelvis syndrome
Preoperative scans rarely tell the whole story. Once the surgeon makes the initial port placements, they frequently encounter a literal battlefield of dense adhesions, excessive visceral fat, or a narrow, deep pubic arch that severely restricts instrument mobility. This anatomical lottery can instantly transform a predictable two-hour prostatectomy into a grueling four-hour chess match. Why does nobody mention how much a patient's unique skeletal structure dictates the operative timeline? If you possess a narrow pelvic basin, your surgeon must navigate a microscopic field with millimeter precision, a reality that naturally inflated the duration of complex radical prostatectomy procedures by sixty to ninety minutes. (Urologists quietly refer to this as the hostile pelvis.)
Frequently Asked Questions
Does a larger prostate size extend how many hours is prostate surgery?
Absolutely, because a severely enlarged gland obscuring the bladder neck demands tedious, bloodless dissection to avoid massive hemorrhaging. While a standard thirty-gram prostate might be excised within 120 minutes, a gland weighing over eighty grams can easily push the operative time past the 240-minute mark. Surgeons must painstakingly separate the massive transitional zone from the peripheral tissue without tearing the fragile urinary sphincter. As a result: gland volume directly correlates with operating room duration, requiring advanced morcellation or specialized morcellation techniques in cases of extreme benign hyperplasia. This anatomical reality means your time under general anesthesia will scale upward alongside the physical grams of tissue requiring removal.
How long will I remain in the post-anesthesia care unit afterward?
Waking up safely takes its own sweet time. You will generally spend between ninety minutes and three hours in the recovery wing while specialized nurses track your vitals and monitor early urine output. The issue remains that clearing the heavy paralytics and gases from your system cannot be hurried, meaning your total theater footprint is much larger than the surgical time alone. Most clinics report that post-operative monitoring requires two full hours before a patient can be safely wheeled to a standard hospital room. But don't expect to remember much of this phase, given the lingering amnesiac effects of modern sedative cocktails.
Does the specific type of anesthesia alter the total procedure length?
The choice between general anesthesia and a combined epidural block changes the preparation phase significantly rather than the cutting time itself. Administering a spinal block adds roughly thirty minutes of precise needle placement before the urology team even enters the room. In short, anesthetic induction adds fixed overhead time to the absolute total room log, meaning a two-hour surgery keeps you in the theater suite for nearly three and a half hours from entry to exit. This administrative and preparatory buffer is standard across ninety-five percent of high-volume oncological centers globally.
A definitive stance on surgical duration
Obsessing over the precise minute count of your upcoming prostatectomy is a manifestation of displaced anxiety that yields zero clinical benefit. We need to stop treating the operating room like a racetrack where speed records matter. If your surgeon takes three hours instead of two, it frequently means they spent an extra sixty minutes meticulously scraping cancer cells off your delicate neurovascular bundles to preserve your quality of life. Superior survivorship and urinary continence are the only metrics that carry real weight, yet patients continue to judge surgical competency by the hands of a clock. Trust the process and demand a meticulous surgeon, not a fast one.