The Anatomical Void: Why Having a Prostate Removed Changes the Internal Landscape Forever
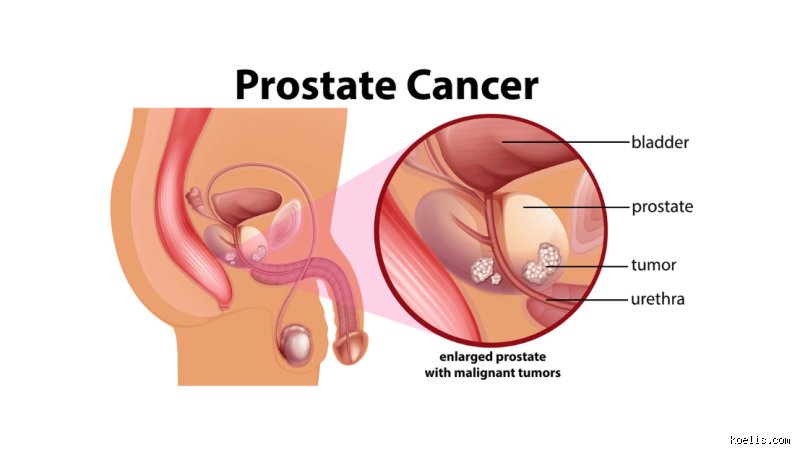
When a surgeon performs a radical prostatectomy, they aren't just taking out a rogue organ; they are essentially re-plumbing your entire lower pelvic region. The prostate sits right at the base of the bladder, hugging the urethra like a tight sleeve, which explains why its absence creates an immediate, cavernous gap in the urinary tract. Doctors must pull the bladder down and stitch it directly to the remaining urethra—a process called vesicourethral anastomosis—and this physical stretching often weakens the internal sphincter's ability to hold back liquid. Most people think of the prostate as just a reproductive gland, but its physical presence acts as a mechanical backstop for the bladder. Without it, the structural integrity of the pelvic floor is compromised, leading to the dreaded "leaks" that haunt post-operative life.
The Neurovascular Bundle Tightrope
The thing is, the nerves responsible for your erections are thin, microscopic threads that cling to the outer surface of the prostate like a spiderweb on a garden hose. Even with the advent of "nerve-sparing" robotic surgery, which became the gold standard around 2005, there is no guarantee that these fibers won't be traumatized by heat, traction, or accidental contact. If these nerves are severed or even just bruised, the signal from the brain to the penis is permanently silenced. But wait, does the surgery always result in total impotence? Not necessarily, yet the recovery period for these nerves can stretch to 24 months, leaving many men in a state of prolonged, frustrating limbo where they feel like a shadow of their former selves.
Rethinking the Urinary Sphincter
It gets tricky when we look at the external urinary sphincter, the muscle you consciously squeeze to stop peeing. After the prostate is gone, this muscle is suddenly the sole gatekeeper of your continence. If it was weak before surgery, perhaps due to age or lack of exercise, you are essentially asking a middle-weight lifter to suddenly hold up a heavyweight bar for 24 hours a day. Honestly, it’s unclear why some men regain full control in weeks while others are still wearing heavy-duty pads two years later, though surgeons in London’s Guy's Hospital have suggested that the functional length of the urethra plays a massive role in this outcome.
Erectile Dysfunction and the Loss of Sexual Spontaneity
The most immediate and visceral downside of having a prostate removed is the death of the "spontaneous" erection. For many, the transition from a natural biological response to a medically managed erection is a psychological blow that no amount of counseling can fully soften. You are no longer just "in the mood"; instead, you are calculating the timing of a Sildenafil dose or, in more severe cases, preparing a penile injection using Alprostadil. Research from the Memorial Sloan Kettering Cancer Center indicates that up to 60% of men experience significant sexual dissatisfaction in the first year following surgery. And then there is the issue of "dry orgasms," because without the prostate and seminal vesicles, there is no fluid to transport sperm, making the climax a purely neurological event without any physical output.
The Psychological Weight of Penile Atrophy
People don't think about this enough, but a penis that doesn't receive regular blood flow due to nerve damage will actually lose length and girth over time. This process, known as cavernosal fibrosis, occurs because the tissue isn't being oxygenated by nocturnal erections anymore. To combat this, many urologists prescribe "penile rehabilitation" involving vacuum pumps or daily low-dose Tadalafil, but the mechanical nature of these solutions often strips the intimacy from a relationship. Is a marriage the same when sex becomes a scheduled clinical procedure? It's a question surgeons rarely have time to answer in a fifteen-minute pre-op consultation.
Orgasmic Incontinence: The Climactic Leak
One of the more jarring and rarely discussed side effects is climacturia, where a small amount of urine is released at the moment of orgasm. This happens because the weakened sphincter cannot withstand the pressure of the pelvic contractions during a climax. While not physically painful, the emotional embarrassment often leads men to avoid intimacy altogether, creating a wedge between partners that has nothing to do with the cancer itself. We're far from a perfect solution here, although some specialists suggest using a tension ring to physically block the urethra during sex.
The Long-Term Battle with Urinary Incontinence
Living with a catheter for the first 7 to 14 days post-surgery is just the beginning of the journey. Once that tube comes out, the reality of stress urinary incontinence hits home—quite literally—as simple acts like coughing, sneezing, or lifting a grocery bag result in a sudden wetness. Data suggests that while 90% of patients eventually achieve "social continence," which usually means using one "safety" pad per day, the road to getting there is paved with expensive absorbent products and a constant mental map of every public restroom in the city. In 2023, a study in the Journal of Urology noted that 15% of men still require more than two pads daily after a year, which often leads to social withdrawal and depression.
The Impact on Social and Physical Activity
The issue remains that having a prostate removed dictates your wardrobe and your hobbies. You might find yourself wearing darker trousers to hide potential accidents or giving up golf because the twisting motion of the swing triggers a leak. I’ve seen men who were once avid marathon runners become sedentary because they couldn't handle the chafing and moisture of pads during long distances. But it’s not just about the physical leakage; it’s the constant vigilance that wears you down, the nagging fear that someone might smell the urine or see a damp spot on your chair. This isn't just a "minor side effect," it is a fundamental shift in how a man moves through the world.
Comparing Radical Surgery to Active Surveillance and Radiation
When we weigh the downside of having a prostate removed, we have to look at what happens if we don't take it out. For many low-risk patients, Active Surveillance (AS) has become the preferred route, involving regular biopsies and PSA blood tests instead of immediate surgery. The logic is simple: why trade your quality of life for a surgery you might not actually need? However, the psychological "sword of Damocles" hanging over your head—knowing you have cancer inside you—can be its own kind of torture. Radiation therapy, specifically Proton Beam Therapy or Brachytherapy, offers an alternative that avoids the immediate surgical trauma but brings its own set of long-term risks, such as radiation cystitis or proctitis.
The Radiation vs. Surgery Trade-off
Radiation generally has a lower immediate impact on continence compared to surgery, yet the sexual side effects tend to show up later and can be more difficult to treat because the blood vessels themselves are damaged by the rays. Surgery is a "big bang" event where you know the damage immediately; radiation is a slow burn where problems might manifest five years down the line. As a result: the choice often boils down to whether you want your complications now or later. There is no "free lunch" in prostate cancer treatment, except that some menus are just more transparent than others.
Common mistakes and misconceptions about prostate removal
The problem is that many patients equate a radical prostatectomy with an immediate, final resolution of their cancer anxieties. People often assume that once the organ vanishes, the PSA score drops to zero and stays there forever. Let's be clear: this is a fallacy. Recurrence happens. Biochemical recurrence occurs in approximately 20 percent to 40 percent of men within ten years of surgery. If a single malignant cell escaped the capsule before the surgeon snipped the tissue, the cancer can resurface in the bone or lymph nodes. Thinking the surgery is a guaranteed "one and done" solution ignores the microscopic reality of oncology.
The myth of the overnight recovery
And then we have the misconception regarding the speed of functional return. Marketing for robotic-assisted laparoscopic prostatectomy often emphasizes "minimal downtime," which leads men to believe they will be continent and potent by their second follow-up appointment. This is rarely the case. While the incisions heal fast, the internal trauma to the neurovascular bundles requires months, sometimes years, to mend. Which explains why expecting dry pants in three weeks is a recipe for psychological distress. Recovery is a marathon of pelvic floor exercises, not a sprint out of the operating theater. You cannot rush the nerves.
The erectile dysfunction misunderstanding
Many believe that "nerve-sparing" techniques ensure a return to pre-operative sexual function. But the reality is far more clinical and cold. Even with the most gifted surgeon, the cavernous nerves are subjected to heat, traction, and inflammation during the procedure. As a result: erectile dysfunction is the norm, not the exception, in the immediate post-operative phase. Approximately 60 percent of men still struggle with spontaneous erections 18 months after the blade has done its work. The downside of having a prostate removed is that "sparing" the nerves does not mean they remain uninjured; it simply means they weren't severed.
The hidden cost: Penile atrophy and structural change
Few surgeons enjoy discussing the literal reduction in size that follows this surgery. It is the conversation nobody wants to have at the golf club. Because the prostatic urethra is removed, the remaining urethra must be pulled up and reattached to the bladder neck. This shortening of the internal plumbing, combined with a lack of regular nocturnal erections, often leads to a measurable loss of penile length. Data suggests that up to 68 percent of patients experience a reduction in penile length of 1.0 to 2.0 centimeters. Is it a fair trade for cancer survival? Most say yes, but the silent mourning for one’s anatomy is a heavy emotional burden that few brochures mention. (Honestly, the psychological impact of this "shrinkage" is frequently more damaging to a man's ego than the incontinence itself).
The expert advice: Pre-habilitation is mandatory
The issue remains that most men wait until they are leaking to start their Kegel exercises. You should be training your pelvic floor months before the surgery. Think of it as training for a physical trauma. We have observed that men who engage in "pre-hab" regain continence up to 30 percent faster than those who start post-operatively. Furthermore, penile rehabilitation using vacuum erection devices or low-dose PDE5 inhibitors should begin almost immediately to maintain tissue oxygenation. In short, do not wait for the body to heal itself; you must actively force the blood back into the tissues before fibrosis sets in permanently.
Frequently Asked Questions
How long does the urinary incontinence actually last?
While every patient is unique, the vast majority of men see a significant improvement within the first six months. Data from large-scale clinical trials indicates that roughly 89 percent of patients achieve social continence—defined as using one or fewer pads per day—by the one-year mark. However, about 5 percent to 10 percent of men will suffer from persistent stress incontinence that requires further surgical intervention like a suburethral sling or an artificial urinary sphincter. The downside of having a prostate removed is that even a small percentage of failure feels like a total failure when it is your underwear that is wet. It requires patience and a very thick skin.
Will I still be able to have an orgasm?
The short answer is yes, though the experience will be fundamentally altered. You will experience what is known as a dry orgasm because the seminal vesicles and the prostate, which produce 95 percent of the ejaculate, are gone. The sensation remains localized in the nerves of the penis and the pelvic floor, so the "climax" still occurs. Yet, some men report a decrease in intensity or even climacturia, which is the involuntary leakage of urine during the peak of sexual pleasure. This happens in about 20 percent to 30 percent of post-prostatectomy patients. It is an ironic twist of biology that the moment of highest pleasure can also be a moment of hygiene crisis.
Is there an increased risk of developing other health issues?
Beyond the immediate surgical risks like blood clots or infection, the long-term shifts in pelvic anatomy can lead to inguinal hernias. Statistics show that men who undergo a radical prostatectomy are nearly 10 times more likely to develop a hernia in the groin area compared to the general population. This usually happens within the first two years following the procedure. There is also the potential for anastomotic stricture, where the new connection between the bladder and urethra scars over and blocks urine flow. While this only affects about 5 percent of cases, it necessitates a painful secondary stretching procedure. Choosing surgery is often a choice between a known enemy and a flock of unpredictable smaller ones.
Taking a stand on the surgical trade-off
Let's stop pretending that a radical prostatectomy is a minor inconvenience on the road to health. It is a massive, life-altering trade of one’s physiological innocence for a chance at longevity. We must acknowledge that for many, the downside of having a prostate removed feels like a betrayal of the masculine self. Yet, the alternative of allowing high-grade localized cancer to metastasize is objectively worse. You are effectively buying years of life at the cost of sexual and urinary spontaneity. I believe we owe patients more honesty about the cluttered reality of recovery rather than polished statistics. Survival is the goal, but we should not have to sacrifice our dignity on the altar of a "clean" PSA score without a fight.