The Anatomy of Removal: What We Are Talking About When the Prostate Vanishes
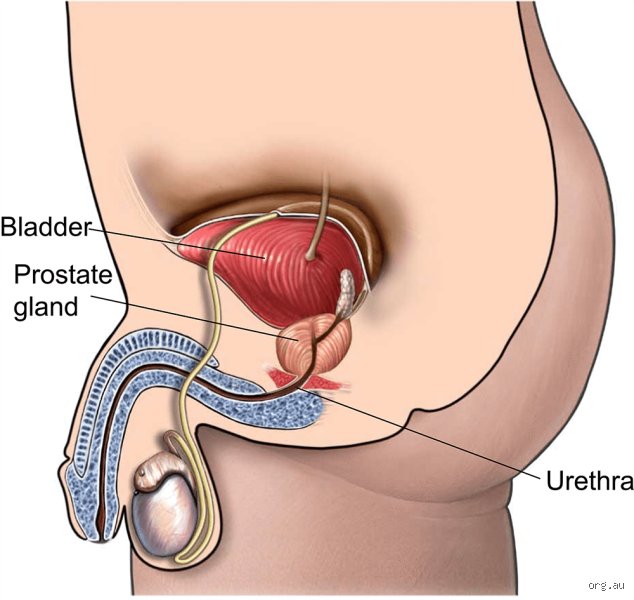
The thing is, people don’t think about this enough: the prostate is not an isolated island sitting loosely inside the pelvis. It surrounds the urethra like a tight collar right at the bladder neck. When a urologist says they are going to completely remove it, they are not just taking a piece of tissue out of a bag. They are cutting a section out of your urinary highway. Because of this strategic location, the surgeon must slice through the urethra, extract the gland, and then pull the bladder down to stitch it back to the remaining urinary tube.
The Walnut and the Web of Nerves
Let us look at the actual geography. In a typical radical prostatectomy, which is the gold standard for full extraction, the goal is total eradication of the organ. But here is where it gets tricky. Hugging the sides of this gland are microscopic cavernous nerve bundles that control erectile function. Can you scrape every single cell of the prostate off those nerves without damaging them? In the mid-1980s, Dr. Patrick Walsh at Johns Hopkins Hospital revolutionized this field by developing the nerve-sparing technique, proving that total removal did not automatically mean a permanent end to intimacy. Yet, if the cancer has breached the prostatic capsule, surgeons must sacrifice those nerves, leaving the patient with a completely different reality.
The Myth of the Partial Radical Surgery
There is a lingering misunderstanding among patients who ask for a "complete removal but leave the outer edge." That changes everything, and honestly, it is a contradiction in terms. When treating malignancy, leaving a margin behind is a recipe for recurrence. In 2024, long-term oncological data confirmed that positive surgical margins—meaning microscopic prostate cells were left at the edge of the resection area—increase the risk of biochemical recurrence by up to 30% within five years. If it is coming out, it has to be a total eviction.
The Surgical Mechanics: How a Radical Prostatectomy Actually Happens
We have moved far beyond the era of massive, belly-slitting incisions that left men hospitalized for a week. Today, the vast majority of complete prostate removals in the United States and Europe are performed using the DaVinci robotic surgical system. The surgeon sits at a console across the room, manipulating robotic arms that enter the patient's abdomen through five or six tiny ports. It looks like science fiction, but the reality is pure, meticulous anatomy. The camera provides a 3D, ten-times magnified view of the pelvis, allowing for a level of precision that open surgery simply could not match.
Robotic Versus Open Total Resection
But does the machine always win? Not necessarily, as experts disagree on whether the robot inherently provides better cancer control. What the robot does guarantee is less blood loss—often under 100 milliliters compared to the 800 milliliters frequently lost during traditional open retropubic surgeries. Think of the pelvis as a dark, deep cup; trying to stitch the bladder back to the urethra at the bottom of that cup with human hands is a nightmare. The robot acts like tiny, hyper-flexible wrists inside that cup, making the reconstruction significantly cleaner. As a result: patients are often up and walking the next morning, which is a massive leap forward from the procedures done in the 1990s.
The Reconnection Phase
Once the prostate and the attached seminal vesicles are bagged and pulled out through one of the small incisions, the patient is left with a literal gap in his urinary tract. This is the moment of truth in the operating room. The surgeon performs an anastomosis, sewing the bladder neck directly to the urethral stump. To allow this delicate new connection to heal without leaking urine into the pelvis, a Foley catheter is inserted through the penis into the bladder. It stays there for anywhere from 7 to 14 days, acting as an internal splint while the body knits itself back together. It is uncomfortable, it is frustrating, but without it, the entire reconstruction would collapse under the pressure of normal urination.
Bladder Control and the New Plumbing: Relearning How to Stay Dry
You cannot cut out a piece of the urinary tract and expect things to work perfectly on day one. When the prostate is completely removed, the internal urethral sphincter, which sits at the base of the bladder and acts as an automatic valve, is gone forever. Now, the entire burden of keeping you dry falls squarely on the external urethral sphincter and the pelvic floor muscles. Imagine a backup goalie who suddenly has to play the entire game because the starter was traded; that is what your pelvic floor is dealing with.
The Incontinence Timeline
When that catheter comes out a couple of weeks after surgery, almost every single man experiences some degree of urinary leakage. It ranges from a few drops when coughing to total, unrestricted flow. I have spoken with patients who were utterly shocked by this, despite being warned beforehand. The timeline for recovery is slow. Statistical models show that while only about 15% of men are dry at the three-month mark, that number jumps to roughly 85% to 90% by the one-year anniversary, provided they actively perform pelvic floor exercises. Except that some men never fully regain control, requiring a second surgery years later to implant an artificial urinary sphincter.
Complete Removal Versus the Alternatives: Radical Subtraction Against Partial Destruction
It is worth asking: do we always need to take the whole thing out? For decades, the medical establishment viewed the prostate as an all-or-nothing proposition. If there was cancer, the whole organ had to go. But we are seeing a massive paradigm shift. The issue remains that a total prostatectomy carries a heavy toll in side effects, leading many researchers to look for ways to destroy the cancer while leaving the healthy parts of the prostate intact.
The Core Differences Between Radical and Focal Procedures
This is where we contrast complete removal with modern focal therapies like High-Intensity Focused Ultrasound or irreversible electroporation. While a radical prostatectomy clears out the entire zip code, focal therapy is a targeted missile strike aimed only at the known tumor within the gland. The trade-off is stark. Complete removal offers a definitive pathological answer—the pathologist looks at the whole prostate under a microscope to confirm the exact stage—whereas focal therapy leaves you with the rest of the organ, which means you need constant, anxious monitoring via MRIs and biopsies to ensure no new tumors pop up elsewhere. We are far from a consensus on which path is superior for intermediate-risk patients, making the decision a deeply personal gamble between quality of life and absolute peace of mind.
The Great Confusion: Common Misconceptions Around Extirpation
Many patients assume that surgical extraction equates to absolute structural emptiness. It does not. The problem is, human anatomy isn't a Lego set where a piece snaps out cleanly leaving pristine boundaries. When a surgeon performs a radical prostatectomy, they extract the entire gland along with the seminal vesicles. But let's be clear: microscopic cellular remnants occasionally linger behind, undetectable to the naked eye. Why does this matter? Because even a few orphaned cells can still secrete Prostate-Specific Antigen, leading to what we call biochemical recurrence.
The Laser Myth: Ablation vs. Elimination
Men often conflate a Holmium Laser Enucleation (HoLEP) or a GreenLight vaporisation with total removal. Huge error. These endoscopic interventions for benign hyperplasia merely hollow out the core to restore urine flow. They leave the peripheral zone completely intact. You still possess a prostate after these procedures, which means the risk of developing malignancy remains completely unchanged. Do not skip your annual screenings just because a laser cleared your urethra.
The Nerve-Sparing Illusion
Can a surgeon truly save your erectile function while pulling out the entire organ? Yes, yet the surgical reality is messy. The cavernous nerves resemble a microscopic spiderweb stuck to the outer casing of the gland. Shaving them off requires millimeter-precision. If the oncological margin is too close, the surgeon must sacrifice those nerves to save your life. Survival trumps erections, always.
The Hidden Impact: Bladder Neck Reconstruction
When the prostate vanishes, a massive anatomical void appears between the bladder and the external urinary sphincter. How do we fix this chasm? Surgeons must physically pull the bladder downward and stitch it directly to the remaining urethra. This is called a vesicourethral anastomosis. It completely alters your internal pelvic architecture. Because of this structural shift, the mechanical angle of urination changes permanently, forcing your pelvic floor muscles to learn an entirely new logic of continence.
The Dynamic of Retrograde Ejaculation
Let us address the literal fluid mechanics of intimacy. Without the seminal vesicles and the prostate, you will experience a dry orgasm. The sensation of pleasure survives because the pudendal nerve remains intact, except that no fluid emerges. Where does it go if some tissue remains? In partial surgeries, the fluid shoots backward into the bladder. In total removals, there is simply zero seminal volume produced whatsoever. It is a strange psychological adjustment that few men are genuinely prepared for.
Frequently Asked Questions
Can a man's prostate be completely removed and still cause a PSA rise?
Yes, this occurs in approximately 20% to 30% of patients within ten years post-surgery. We track this via ultra-sensitive blood tests where any value above 0.2 nanograms per milliliter signals trouble. This metric usually implies that microscopic cells survived outside the surgical margins before the knife even touched your skin. As a result: salvage radiation therapy becomes the next logical frontline defense to sterilize the pelvis.
Will my sexual function return to normal after radical surgery?
Normal is a relative term here, given that erectile recovery timelines stretch between 12 and 24 months. Statistics show that only 40% to 60% of men regain natural, penetration-grade erections without the assistance of pharmacological aids or vacuum devices. Much depends on your pre-operative baseline health, your age, and whether the dual nerve bundles were successfully preserved. (The younger you are, the better your microscopic nerve pathways bounce back from surgical trauma).
How long does urinary incontinence typically last after total excision?
Most patients experience significant leaking immediately after the urinary catheter is pulled out at week two. However, clinical data indicates that 85% of men achieve satisfactory dryness by the one-year milestone through rigorous pelvic floor physical therapy. A persistent 5% to 10% of cases might require a secondary surgical implant like an artificial urinary sphincter if the leakage remains profound. Is it frustrating to wear protective pads for months while your body heals? Absolutely, which explains why pre-operative Kegel exercises are heavily emphasized by modern urological teams.
A Definitive Stance on Radical Intervention
We need to stop viewing the total eradication of this gland as a simple plug-and-play cure without consequence. The anatomical reality proves that completely removing a man's prostate is a life-altering trade-off between oncology and quality of life. It is an aggressive, necessary violence against localized cancer that demands respect. Medical literature confirms that excellent survivability rates come at a direct cost to baseline urinary and sexual mechanics. Do not let clinical optimism blind you to the demanding physical rehabilitation required afterward. In short, choose your surgeon based on their volume of successful reconstructions, not just their ability to cut the tumor out.