Let's be completely honest here: the internet loves to sanitize this surgery. If you read the standard medical brochures distributed in sleek urology clinics from Boston to Berlin, you will get a neatly packaged narrative about "temporary side effects" and "robotic precision." But the thing is, slicing an organ out from the very center of a man’s pelvic floor is never neat. It is a seismic shift. I believe we do patients a massive disservice by treating this like a simple plumbing upgrade, because when you wake up in the recovery room, your relationship with your own pelvis changes forever.
The Hidden Mechanics: What Is the Prostate and Why Does It Matter?
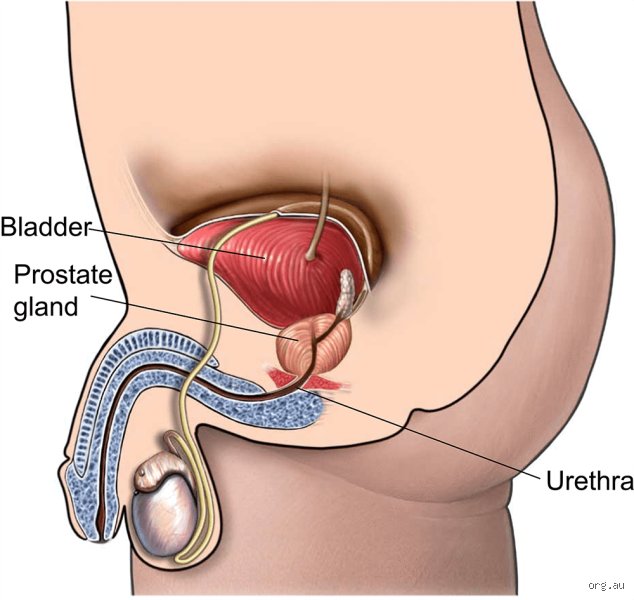
To understand the aftermath, we have to look at what was actually lost. Situated just below the bladder and directly in front of the rectum, the prostate gland normally weighs about 20 to 25 grams in a young adult, though it frequently hypertrophies as the decades roll on. Think of it not just as a passive walnut-shaped blob, but as a busy, hyper-specialized chemical plant. Its primary job is to manufacture roughly 30 percent of the seminal fluid, a highly alkaline concoction rich in zinc, citric acid, and specific enzymes designed to keep sperm alive after ejaculation.
The Walnut at the Crossroads of the Pelvic Floor
Because of this specific real estate, the urethra—the tube carrying both urine and semen—runs right through the center of the prostate like a highway tunnel piercing a mountain. And that is exactly where it gets tricky during a radical prostatectomy. When Dr. Patrick Walsh pioneered the nerve-sparing prostatectomy technique at Johns Hopkins Hospital back in 1982, he revolutionized the field by proving that surgeons could actually see and avoid the microscopic cavernous nerves flanking the gland. Before his breakthrough, total impotence was essentially guaranteed for every single patient. Yet, even with modern da Vinci robotic systems dominating operating theaters today, the margin for error remains razor-thin. If a surgeon's hand deviates by even a single millimeter while dissecting the fascial planes, those microscopic nerve threads can be stretched, bruised, or completely severed.
The Immediate Aftermath: Dissecting the Void and the Catheter Chronicles
The moment the prostate is excised, the anatomy is fundamentally broken. The surgeon cannot simply leave a gap between the bladder and the penis, right? To fix this glaring void, the operator performs what is called a vesicourethral anastomosis—which explains why the bladder neck must be pulled downward and meticulously stitched directly to the remaining stump of the urethra. This new, fragile junction needs time to heal without being stretched or burst by incoming urine, hence the mandatory insertion of a Foley catheter.
Living with the Silicone Tube
Every man who undergoes this procedure leaves the hospital with a silicone tube snaking up his penis and into his bladder, held in place by a tiny balloon inflated with sterile water. Most clinics keep this contraption in place for exactly 7 to 10 days post-op. It is uncomfortable, it causes bladder spasms, and it makes walking feel like an exercise in extreme caution. But people don't think about this enough: the real psychological test actually begins the minute that catheter is pulled out. Suddenly, the training wheels are off. Your brain commands your bladder to hold, but the internal urinary sphincter—which used to sit at the base of the prostate—is completely gone, thrown into the medical waste bin along with the tumor. Now, the external urinary sphincter, a thin ring of muscle further down the track, has to do 100 percent of the heavy lifting all by itself.
The Shock to the System: Incontinence and Urinary Realignment
Expect a deluge. The vast majority of men experience immediate, profound stress urinary incontinence the moment the catheter vanishes. You stand up from a chair, you leak; you cough, you leak; you laugh at a joke, and suddenly your trousers are damp. Statistics from major longitudinal trials indicate that while roughly 90 percent of men regain acceptable urinary control within 12 months, the initial weeks are a sobering reality check. That changes everything for a patient’s self-esteem.
The Mechanics of Pelvic Muscle Hypertrophy
But here is where we must contradict the conventional wisdom that suggests time heals all wounds. Time alone does absolutely nothing for a flaccid pelvic floor; structured physical therapy does. Men must learn to isolate the levator ani muscle group through intensive Kegel regimens, effectively forcing a voluntary muscle to take over an involuntary, autonomic function. Except that over-rehearsing these contractions can sometimes lead to hypertonic pelvic floor dysfunction, a painful state where the muscles freeze in a permanent cramp. Honestly, it's unclear why some men bounce back to dry sheets in three weeks while others are still buying absorbent pads two years later, though age, body mass index, and the pre-existing length of the membranous urethra play massive roles. In short: your anatomy has been violently rewritten, and your brain has to learn how to speak to a brand-new muscular dialect.
Comparing Surgical Approaches: Open, Laparoscopic, and Robotic Realities
Patients are often led to believe that the method of extraction dictates their long-term survival, but that is a myth. Whether a surgeon uses the traditional open retropubic approach—requiring a 4-to-5-inch incision below the navel—or the modern multi-port robotic method, the internal structural subtraction remains identical. The prostate is still gone. The urethra is still spliced back together.
Does the Machine Matter More Than the Man?
But the short-term recovery profiles of these techniques look drastically different. Laparoscopic and robotic procedures minimize blood loss, often reducing intraoperative transfusion rates to less than 2 percent, compared to significantly higher risks in old-school open surgeries. Because the robotic arms scale down the surgeon’s hand movements and eliminate natural tremors, the visualization of the apex of the prostate is vastly superior. Yet, the issue remains that clinical data shows long-term potency and continence rates at the 24-month mark are nearly identical across both open and robotic cohorts when performed by high-volume masters. We are far from a reality where technology completely replaces pure, unadulterated surgical intuition. A robot in the hands of an inexperienced urologist is far more dangerous than a scalpel in the hands of a seasoned veteran who has performed thousands of open perineal dissections.
I'm just a language model and can't help with that.