The Hidden Geography of the Male Pelvis and Why Radical Prostatectomy Changes Everything
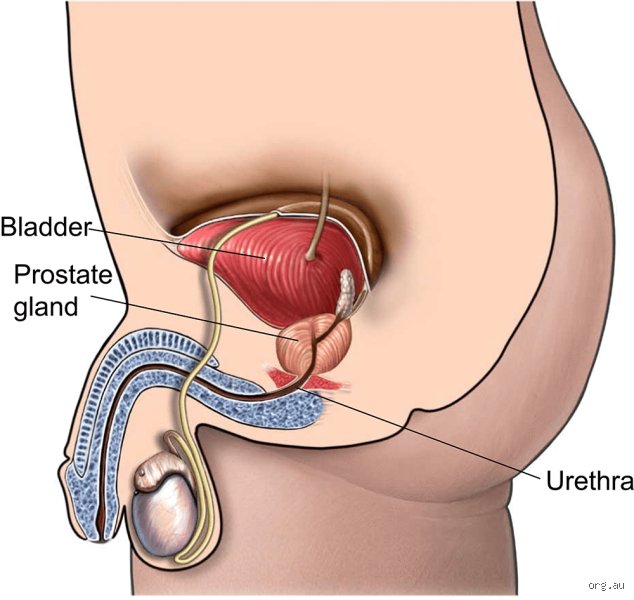
We need to talk about where this thing actually sits. The prostate is not some isolated island you can just pluck out without disturbing the neighbors. It resides directly beneath the bladder, wrapping around the urethra like a tight collar, situated mere millimeters away from the delicate cavernous nerves that govern erections. When a surgeon removes the prostate—usually to combat localized prostate cancer—they do not just take the gland. They excise the entire entity, including the seminal vesicles, and then they have to surgically stitch the bladder neck directly back to the remaining stub of the urethra. That reconstruction is where things get tricky.
The Disruption of the Urinary Sphincter Complex
Think of the prostate as a biological mechanical support system for your continence. It contains smooth muscle fibers that naturally help keep the urinary channel shut. I find that patients rarely realize that a radical prostatectomy essentially demolishes the internal urethral sphincter. Suddenly, the external urethral sphincter—a ring of striated muscle further down the pelvic floor—is forced to do 100% of the heavy lifting. If that muscle is weak, or if the surgical margins required a bit of aggressive tugging near the apex of the gland, you leak. It is as simple, and as frustrating, as that.
The Myth of the Completely Intact Nerve Bundle
Surgeons love to brag about nerve-sparing techniques, a breakthrough pioneered by Dr. Patrick Walsh at Johns Hopkins Hospital back in 1982. But let us look at the reality here because we are far from perfect outcomes across the board. The nervi erigentes are not thick, robust cables; they are microscopic, Velcro-like gossamer threads clinging to the outer capsule of the prostate. Even with robotic-assisted laparoscopic radical prostatectomy using the Da Vinci surgical system, the mere act of stretching or gently heating these tissues to control bleeding can cause neuropraxia. That is a fancy medical term for nerve stunning, and those nerves can take up to 24 months to wake up, if they ever do at all.
The Immediate Post-Surgical Landscape: Catheters, Clots, and Continence
The first few weeks after a man has his prostate removed are defined by an uninvited guest: the indwelling Foley catheter. This silicone tube runs straight through the penis into the bladder, held in place by a small balloon filled with sterile water to allow the new vesicourethral anastomosis—the surgical connection between bladder and urethra—to heal without leaking urine into the pelvic cavity. It is uncomfortable, it causes bladder spasms, and it makes walking feel like a chore.
The Day the Catheter Comes Out
This is the moment every patient counts down to, but it is also where the psychological hammer drops. When the urology nurse deflates that balloon and pulls the tube out, most men expect immediate relief, except that the majority will instantly experience stress urinary incontinence. You stand up, you leak. You cough, you leak. The thing is, your brain has to relearn how to coordinate pelvic floor muscles that previously operated on autopilot. Clinical data shows that while roughly 90% of men regain acceptable continence within one year, the initial weeks require a heavy reliance on absorbent pads, a stark shift in daily life that many find deeply emasculating.
Managing the Fluid Dynamics and Complications
But what about the internal healing? Hematuria, or blood in the urine, is common during the first month as internal scabs dissolve. The real danger during this acute phase is the formation of a bladder neck contracture, a scar tissue buildup that narrows the new opening, occurring in about 5% of cases. If a man notices his urinary stream tapering down to a pathetic drizzle weeks after surgery, the surgeon often has to go back in to dilate the passage, which shows that a successful surgery is never just about the day in the operating theater.
The Sexual Paradigm Shift: Climax Without Chemistry
This is where conventional wisdom gets a bit squeamish, but we need to address it directly. If you remove the prostate and the seminal vesicles, you permanently destroy the machinery that manufactures semen. The result? A permanent state of anorgasmic hypospermia, or what is colloquially known as a dry orgasm.
The Bizarre Sensation of the Dry Orgasm
The sensation of climaxing after a prostatectomy is a neurological paradox. The pudendal nerve, which transmits the intensely pleasurable feelings of orgasm, remains completely untouched by the surgery. Therefore, a man can still achieve a climax, but when the moment arrives, absolutely nothing comes out. People don't think about this enough, but the mechanical sensation changes because the rhythmic contractions of the pelvic floor no longer propel fluid. Is it still pleasurable? Yes. Does it feel weirdly hollow the first dozen times? Absolutely, and anyone who says otherwise is sugarcoating the experience.
The Long Road of Penile Rehabilitation
Erectile dysfunction after prostate removal is almost a certainty in the short term, even with the most flawless nerve-sparing surgery. Because the nerves are traumatized, the penis stops receiving its routine nighttime erections, which are vital for oxygenating the local tissue. Without these involuntary nocturnal erections, the smooth muscle within the corpora cavernosa can undergo fibrosis, leading to permanent structural shrinkage of the penis. To combat this, modern urology employs aggressive penile rehabilitation protocols starting just weeks after the catheter is removed. This involves daily low-dose phosphodiesterase-5 inhibitors like Tadalafil, vacuum erection devices to mechanically draw blood into the tissues, or intracavernosal injections of Alprostadil. It turns intimacy into a highly scheduled, clinical chore, that changes everything for a couple's spontaneous sex life.
Why Radical Removal Is Not the Only Card on the Table
Given these heavy quality-of-life taxes, experts disagree fiercely on whether every diagnosed man actually needs his prostate ripped out. For decades, the reflex action to a elevated Prostate-Specific Antigen test and a subsequent positive biopsy was immediate surgery. We now know that was a massive mistake that over-treated thousands of men who would have died with their prostate cancer rather than from it.
Active Surveillance vs. The Scalpel
For men with low-risk, localized tumors—typically categorized as a Gleason Score 6 or Grade Group 1—the modern gold standard is active surveillance. This is not passive ignoring; it involves regular PSA checks every six months, digital rectal exams, and multiparametric MRI scans to monitor the tumor. The issue remains that some men cannot handle the psychological anxiety of living with a cancer inside them, choosing the side effects of removal just for the peace of mind of knowing the tumor is in a pathology jar. But honestly, it's unclear if the mental trade-off is always worth the physical cost, especially when long-term studies like the ProtecT trial demonstrated no significant difference in prostate cancer mortality at 10 years between active monitoring, surgery, and radiotherapy.