The Post-Prostatectomy Anatomy: What Happens Inside When the Prostate Leaves
To understand why a permanent bag is a myth, we must look at what the surgeon actually changes. The prostate sits directly beneath the bladder, wrapping around the urethra like a small, walnut-sized collar. When a urologist performs a radical prostatectomy—whether using the modern DaVinci robotic surgical platform at Johns Hopkins or traditional open methods—they excise this entire glandular structure along with the seminal vesicles.
The Urinary Reconnection Strategy
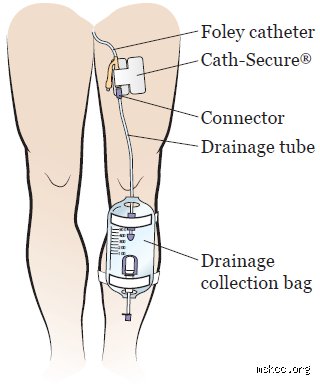
Once the tissue is out, a gap remains between the bladder neck and the remaining urethral stump. The surgeon performs what is called a vesicourethral anastomosis. In plain English? They pull the bladder down and stitch it directly back to the urethra to restore a continuous pipeline for urine. Because this delicate new junction needs time to heal without being stretched or leaked on, a silicone Foley catheter is threaded through the penis into the bladder. It drains urine into a temporary leg bag for roughly a week or two. That is the only bag you will handle. And quite honestly, comparing a two-week temporary tube to a permanent stoma bag is like comparing a twisted ankle to an amputation; we are far from the same medical universe.
The Misconception of the Stoma Bag
So where does this persistent fear come from? It usually stems from confusion between urological procedures and colorectal surgeries, such as those for advanced rectal cancer where a colostomy stoma is genuinely required. The prostate is intimate neighbors with the rectum, separated only by a thin layer of tissue called Denonvilliers' fascia. Because of this proximity, patients assume the bowels are rerouted. Except that they are not. Unless a tumor has aggressively invaded the rectal wall—a scenario that top oncology centers catch via 3T multiparametric MRI scans long before the scalpel touches skin—the gastrointestinal tract remains entirely untouched.
Catheters, Continence, and the Real Mechanics of Urinary Drainage
The thing is, dealing with the temporary urinary catheter is where it gets tricky for most men. It is not painful, but it is undeniably annoying. The device uses a tiny, 10cc sterile water balloon inflated inside the bladder to keep it anchored in place. Urine flows continuously via gravity into a drainage bag strapped to the calf during the day, or a larger 2,000mL bedside bag at night.
Managing the Short-Term Plumbing
The issue remains that patients treat the catheter like a fragile bomb. It is sturdier than you think. You can walk, sit, and sleep, though a sudden tug will remind you of its presence rather sharply. At clinics like the Cleveland Clinic, post-op protocols emphasize early ambulation—getting out of bed on day one—even with the bag attached. Why? Because movement prevents deep vein thrombosis. But what about leaks? It is completely normal to see a bit of blood-tinged urine or spasms around the tip of the penis, especially during bowel movements. It does not mean the surgical reconstruction is failing; it just means the bladder muscle is irritated by the foreign plastic tube.
The Day of Liberation: Catheter Removal
When that one-to-two-week milestone hits, you head back to the urology clinic for a cystogram or a simple voiding trial. The nurse deflates the internal balloon with a syringe and slides the tube out. The process takes roughly five seconds and feels like a weird, cold sensation—not agonizing pain. Once that catheter is gone, your reliance on any external plumbing officially ends. But that changes everything regarding your daily routine, because now a new challenge takes its place: temporary incontinence.
Navigating the Immediate Aftermath of Becoming Bag-Free
Do not expect to dry up instantly the second the tube slides out. The prostate used to assist with urinary control by providing mechanical resistance against the bladder neck. Without it, the pelvic floor muscles and the external urethral sphincter have to do 100% of the heavy lifting. Did you know that nearly 90% of men experience some degree of stress urinary incontinence immediately after catheter removal?
The Transition to Absorbent Pads
Instead of a bag, you will be wearing protective underwear or absorbent male guards, such as Depend or TENA pads, inside your regular briefs. In the first few weeks, you might burn through three to five heavy pads a day just from coughing, standing up, or laughing. It is discouraging. You will wonder if the surgeon messed up. But experts disagree on how fast control returns, proving that healing is a non-linear journey dictated by individual anatomy and the length of your membranous urethra. It is a slow re-education of the body, not a permanent disability.
The Power of Pelvic Floor Physical Therapy
To speed up this recovery, standard medical guidelines recommend Kegel exercises, which isolate the levator ani muscle group. Ideally, you should start these weeks before the operation at a specialized pelvic physical therapy center. Think of it like training for a marathon; you would not run 26 miles without hitting the treadmill first, would you? Contracting these muscles for 10 seconds at a time, 30 times a day, builds the structural back-up system needed to stop leaks dead in their tracks, eventually reducing your pad reliance to zero over three to six months.
Comparing Radical Prostatectomy Recovery to Other Urological Surgeries
To put the prostate removal narrative into perspective, we have to look at what happens when a bag actually *is* mandatory. This helps dismantle the anxiety surrounding prostatectomies by highlighting what you are avoiding.
Prostatectomy vs. Radical Cystectomy
People don't think about this enough: the true "urostomy bag" surgery is a radical cystectomy, which is the complete removal of the urinary bladder, usually due to aggressive bladder cancer. In that scenario, surgeons must create an ileal conduit. They take a piece of your small intestine, fashion it into a pipeline from the ureters to the outside of the abdomen, and create a permanent stoma. As a result: the patient must wear an adhesive, external urostomy pouch for life to collect urine. It is an intensive lifestyle shift. With prostate removal, your bladder stays right where it belongs, meaning your natural anatomy for waste elimination is preserved.
Robot-Assisted vs. Perineal Approaches
The surgical technique chosen also influences your immediate post-op comfort, though not your need for a bag. A robotic-assisted laparoscopic prostatectomy (RALP) uses five tiny incisions across the abdomen, resulting in minimal blood loss—often under 150mL—and a faster internal healing rate for the bladder connection. In contrast, the older perineal approach, which cuts between the scrotum and anus, carries a slightly higher risk of transient bowel disturbance due to the proximity of the rectal nerves. Yet, regardless of whether the surgeon goes through the abdomen or the perineum, the urinary tract is always stitched back together organically, leaving the gastrointestinal tract intact and rendering any fecal or urinary collection bags entirely unnecessary for standard recoveries.
Common mistakes and misconceptions about post-prostatectomy plumbing
The myth of the permanent external collection pouch
Men facing surgery frequently conflate a radical prostatectomy with a colorectal resection, leading to the terrifying assumption that they will be strapped to an ostomy pouch forever. Let's be clear: prostate cancer surgery does not involve a colostomy or an ileostomy. The digestive tract remains completely untouched during this intervention. The confusion stems from a fundamental misunderstanding of pelvic anatomy, where the bladder and bowel are separate entities. Because the prostate surrounds the urethra, the surgeon must reconnect the bladder neck directly to the urinary channel after removing the gland. This temporary disruption requires an internal catheter, not an external bag attached to your abdomen. Yet, patients routinely panic, thinking they will need to wear a bag after prostate removal for the rest of their lives, mixing up urinary drainage with fecal diversion.
Conflating the temporary catheter with an ostomy bag
During the immediate convalescence period, you will leave the hospital with a Foley catheter in place, which drains urine into a collection bag strapped to your leg. This temporary drainage system is not permanent, nor is it an ostomy. The problem is that many men view this two-week recovery tool as a permanent sentence. It is merely a structural splint. It allows the delicate vesicourethral anastomosis, the new connection between your bladder and urethra, to heal securely without leaking fluid into the pelvic cavity. But historical data shows that nearly thirty percent of patients experience significant anxiety simply because they mistake this short-term postoperative necessity for a lifelong requirement. Do you have to wear a bag after prostate removal permanently? Absolutely not, as the catheter typically vanishes within seven to fourteen days once the internal tissue knit together safely.
Overestimating the severity of long-term urinary incontinence
Another widespread fallacy is that post-surgical leaking is both total and irreversible, forcing a reliance on adult diapers forever. While transient stress incontinence affects a vast majority of men immediately after catheter removal, the human body adapts with remarkable resilience. The external urinary sphincter, a muscular ring located just below the prostate, takes over the full burden of continence. Except that this muscle requires time, physical therapy, and patience to regain its strength after the trauma of surgery. Believing that a mild leak equals total structural failure causes unnecessary despair. Clinical registries indicate that over eighty-five percent of patients regain satisfactory control within twelve months, rendering the fear of permanent, heavy pad usage largely unfounded for the vast majority of recovering individuals.
The neurological timeline and pelvic floor calibration
The hidden role of the pudendal nerve network
Surgeons talk endlessly about plumbing, but the real mastermind behind your dryness is the delicate neurological architecture governing the pelvic floor. When the prostate is excised, the microscopic nerves surrounding the bladder neck experience a form of surgical stunning known as neuropraxia. This temporary paralysis disrupts the biofeedback loop between your brain and the external sphincter muscle. As a result: your bladder might contract unexpectedly, or the sphincter may fail to tighten when you cough, laugh, or lift something heavy. Pelvic floor physical therapy, specifically targeted Kegel exercises guided by biofeedback technology, acts as a recalibration tool for these stunned pathways. It is not just about squeezing muscles blindly; it is about retraining the brain to fire the correct motor units at the exact millisecond pressure rises in the abdomen. This intricate neural recovery explains why continence returns in gradual waves rather than overnight, a factor that requires meticulous tracking during your medical follow-ups.
Frequently Asked Questions about post-surgical urinary management
How long must I use the urinary drainage bag after my operation?
The standard duration for wearing the temporary Foley catheter and its accompanying leg collection bag ranges between seven and fourteen days. Clinical protocols dictate this timeline because the newly created connection between the bladder and the urethra requires uninterrupted time to become watertight. Urologists typically perform a cystogram, a specialized imaging test, if they suspect healing is delayed before pulling the tube. Data indicates that ninety-two percent of men successfully have their catheters removed at their first two-week postoperative appointment. Leaving the device in place for longer periods exponentially increases the risk of symptomatic urinary tract infections and urethral irritation.
Will I leak urine immediately after the temporary catheter is removed?
Yes, structural leakage is a near-universal experience during the initial hours and days following the removal of your surgical catheter. When the balloon is deflated and the tube slides out, the external sphincter muscle is suddenly forced to bear the entire hydrostatic pressure of your bladder without assistance. You can expect to use two to four absorbent pads per day during this acute phase of recovery. However, urological statistics show rapid improvement within the first six weeks as localized swelling subsides and anatomical structures settle. This initial vulnerability is entirely normal and does not indicate that your surgery was unsuccessful or that your continence is permanently compromised.
Are there permanent alternatives if my bladder control does not return?
In the rare event that severe urinary incontinence persists beyond one full year, highly effective surgical interventions can permanently restore dryness without requiring an external bag. The two primary gold-standard options are the male transobturator sling and the artificial urinary sphincter, which boasts a ninety percent patient satisfaction rate in clinical trials. The sling acts as a supportive hammock that compresses the urethra during physical exertion, while the artificial sphincter uses an implantable fluid cuff managed by a small pump hidden in the scrotum. Which explains why nobody needs to live in fear of permanent saturation; modern medicine offers mechanical solutions that replicate natural continence beautifully if biological healing falls short.
A definitive stance on post-prostatectomy reality
We need to dismantle the archaic, fear-driven narrative that surrounds prostate removal and replace it with clinical reality. The anxiety regarding whether you have to wear a bag after prostate removal is an phantom menace born from poor medical literacy and old wives' tales. You will handle a temporary catheter for a fortnight, and you will likely navigate a few months of pesky dripping that requires pads, but you will not be saddled with a permanent abdominal pouch. In short: the modern surgical approach prioritizes anatomical preservation, and our medical arsenal for managing incontinence is far too advanced for any man to be left soaking in despair. (Of course, individual anatomy and tumor size can occasionally complicate things, but those outliers should not dictate the general expectation.) Do not let the terrifying image of an ostomy bag deter you from a potentially life-saving cancer eradication. Trust the mechanics of your pelvic floor, commit aggressively to your physical rehabilitation, and understand that temporary leakage is merely a brief pit stop on your journey back to total dryness.