The Anatomy of Desire: Why We Confuse a Walnut-Sized Gland with the Soul
For decades, medical textbooks treated the prostate as a mere secretory organ, a small gland nestled just below the bladder, quietly churning out the seminal fluid that transports sperm. But we’ve done a massive disservice to men by reducing their sexual identity to this single piece of flesh. The thing is, Western culture has conflated erectile mechanics with the capacity for affection, creating a fragile framework where a surgical scalpel can seemingly slice away a man's ability to connect. It is a biological misunderstanding with devastating emotional consequences.
The Real Role of the Prostate in the Male Feedback Loop
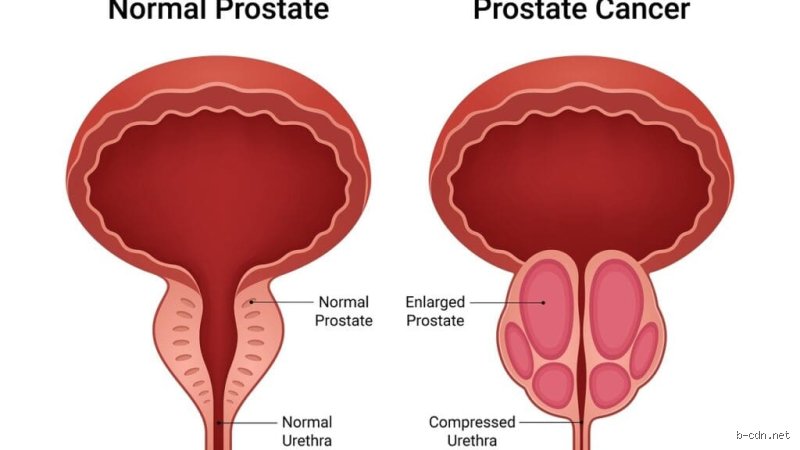
Let’s look at the numbers because the reality is stark. In 2024, the American Cancer Society estimated that over 299,000 men would be diagnosed with prostate cancer in the United States alone. That is nearly 300,000 households forced to confront the intersection of survival and sexuality. When a surgeon performs a radical prostatectomy—the complete removal of the gland—they aren't just removing a tumor; they are disrupting a complex neural highway. The cavernous nerves, which run like microscopic spiderwebs along the surface of the prostate, are the very triggers for penile erection. If those nerves are bruised or severed, the physical response stalls. But does the desire vanish? We’re far from it, and that changes everything.
The Psychological Echo Chamber of Surgical Trauma
Here is where it gets tricky. A man sitting in a urologist's office in Boston or London hears the word "cancer" and his survival instinct kicks in, but the lingering ghost in the room is always impotence. Dr. John Mulhall, a renowned sexual medicine specialist at Memorial Sloan Kettering, has noted that the pre-operative anxiety regarding sexual death often rivals the fear of the disease itself. Why? Because we have conditioned men to believe that their worth, their tenderness, and their validity as a partner reside entirely in their pelvic floor. It is a lie, of course. Yet, when the post-op reality hits and the body refuses to cooperate, the psychological withdrawal can be paralyzing, leading to a state of pseudo-grief that freezes intimacy long before the nerves even have a chance to regenerate.
Beyond the Mechanical Monarchy: Decoding Intimacy After a Radical Prostatectomy
To understand intimacy without a prostate, we must first dethrone the erection. For generations, sexology focused almost exclusively on the penetrative model—a rigid, linear progression from arousal to insertion to climax. But when a radical prostatectomy removes the physical machinery responsible for fluid production, the entire sequence is disrupted. The result is a phenomenon known as a dry orgasm, where the climax occurs with regular intensity but without any ejaculate. And honestly, it’s unclear why this shocks so many men, considering that the sensation of pleasure is governed by the central nervous system, not the fluid itself.
The Chemistry of Connection Versus Pelvic Mechanics
The human brain remains the primary sexual organ, a fact that becomes glaringly obvious in the recovery room. When the prostate is gone, the body’s hormonal architecture—specifically the production of testosterone in the testes—remains largely untouched, unless the patient is undergoing androgen deprivation therapy. This means the raw drive, the hunger for connection, and the capacity for deep emotional attachment are completely intact. Yet, if a man views his body as broken, his brain will refuse to release the oxytocin and dopamine necessary to foster closeness. It is a self-fulfilling prophecy of isolation. I have seen men give up on relationships entirely because they couldn't separate their ability to love from their ability to perform on command.
The Timeline of Nerve Recovery and the Myth of Spontaneous Healing
Nerve regeneration is a agonizingly slow process, moving at a glacial pace of about one millimeter per day. This means that after a nerve-sparing surgery, a man might wait anywhere from 12 to 24 months to see a return of natural erections. It is a grueling test of patience. During this interim period, couples often find themselves in an intimacy desert, terrified to touch because touch might lead to an expectation that cannot be met. But who dictated that touch must always have an endgame? If a couple cannot navigate the space between affection and erection, the relationship will fracture, not because of the surgery, but because their definition of love was too narrow to begin with.
The Neuroscience of the Heart: Why Emotional Resilience Outlasts Physical Anatomy
There is a sharp divide in the medical community regarding how we counsel patients post-surgery. Some urologists focus entirely on pills and pumps, treating the penis like a faulty plumbing fixture that just needs the right wrench. But the issue remains that mechanical fixes do nothing to repair a bruised ego or a disconnected partnership. True resilience after prostate removal relies on a concept known as neuroplasticity—the brain's ability to reorganize itself and find new pathways to pleasure and emotional fulfillment.
How the Brain Re-maps Pleasure Zones Post-Surgery
When the traditional pathways are damaged, the brain can actually become more sensitive to other stimuli. This isn't just wishful thinking; it is verified neurology. Men who have undergone prostatectomies often report that areas of their body previously ignored—the neck, the chest, the inner thighs—become highly eroticized. The body adapts, finding alternative routes to express and receive pleasure. Yet, this re-mapping can only happen if a man allows himself to explore his body without shame or frustration. If he remains fixated on what was lost, he will miss the entirely new sensory landscape waiting to be discovered.
The Nuance of the Partner's Perspective in the Recovery Journey
We rarely talk about the partners, which is a massive oversight. A study published in the Journal of Sexual Medicine revealed that a partner's adaptation to post-prostatectomy changes is the single biggest predictor of a man's long-term sexual satisfaction. If the partner views the lack of an erection as a personal rejection or a permanent tragedy, the man's recovery stalls. But when a partner approaches the situation with curiosity and warmth, the pressure dissipates. In short: love doesn't require a prostate, but it absolutely requires a willingness to abandon the old script and write a new one together, even when the ink feels faint.
The Great Divide: Re-learning Love in an Age of Pharmacological Fixes
We live in a culture obsessed with the quick fix, where a blue pill is supposed to solve every intimate ailment. Following a prostatectomy, drugs like sildenafil or tadalafil are routinely prescribed as part of a penile rehabilitation protocol to keep blood flowing to the tissues. They are incredibly useful tools, but they are not a substitute for desire, nor can they manufacture love. They are merely facilitators of a physical state, completely useless if the emotional connection between two people has been allowed to atrophy.
The Illusion of the Medicalized Relationship
Where it gets dangerous is when couples rely solely on these medical interventions to salvage their intimacy. An injection or a vacuum pump can create rigidity, yes, but it cannot create closeness. In fact, many men find the clinical nature of these devices to be a total mood-killer, turning what should be an act of vulnerability into a scheduled chore. As a result: the physical apparatus might work perfectly while the emotional distance between the partners grows wider by the day. It is a stark reminder that a functioning penis does not guarantee a functional relationship, a nuance that conventional wisdom often ignores in its rush to declare a patient "cured" based on physical metrics alone.
Common misconceptions holding men back
The phantom orgasm myth
Many patients equate ejaculation with the summit of sexual pleasure. The problem is, they mistake the cargo for the vessel. After a radical prostatectomy, the fluid factory is permanently shuttered. Yet, the neurological scaffolding responsible for climax remains entirely intact. You will experience what medicine terms a "dry orgasm," which sounds inherently dusty but feels remarkably undiminished. Because the pudendal nerve still fires on all cylinders, the rhythmic pelvic contractions happen right on cue. It is a psychological hurdle, not a physical deficit.
The timeline trap
Men often expect their libido to bounce back like a rubber band within weeks of surgery. Let's be clear: nerve regeneration operates at a glacial pace of roughly one millimeter per day. Impatience routinely kills romance before the anatomy even has a chance to heal. If you track progress by the weekend, you will spiral into performance anxiety. A damaged nerve requires up to 24 months to fully recover its conductive mojo. Can a man love without his prostate while waiting for this biological crawl? Absolutely, provided he divorces intimacy from immediate rigid erections.
The testosterone confusion
The prostate does not manufacture masculinity. It is merely a glandular transit station for semen production. Your testicles, assuming they were not part of a broader oncological sweep, continue pumping out chemical vitality exactly as before. Do not confuse plumbing issues with a drop in your primal drive. Your desire stays hardwired in your brain, completely unaffected by the missing pelvic architecture.
The overlooked variable: Pelvic floor rehabilitation
The power of physical therapy
Urologists routinely prescribe Kegels for urinary incontinence, but they rarely mention the sexual payoff. Except that strengthening the levator ani muscle group is your fastest ticket to erectile recovery. Increased blood flow to the remaining penile structures relies heavily on this muscular sling. Think of it as manual override for a compromised nervous system. Targeted pelvic floor therapy boosts recovery rates by a staggering 35 percent compared to men who simply wait out the clock. It requires discipline, but the structural dividend is massive.
Frequently Asked Questions
Can a man love without his prostate and maintain a functional erection?
Yes, though the immediate post-operative landscape usually requires therapeutic scaffolding. Clinical data indicates that between 40% and 85% of men regain functional erections within two years, depending heavily on whether a nerve-sparing surgical technique was utilized. Age also dictates the recovery curve, with patients under 60 showing significantly higher rates of spontaneous tumescence. Early intervention using PDE5 inhibitors or vacuum erection devices keeps the penile tissues oxygenated during the lull. As a result: penile rehabilitation prevents structural atrophy while the autonomic nerves slowly repair themselves.
How does prostate removal alter the subjective sensation of intimacy?
The emotional architecture often deepens because the mechanics are no longer on autopilot. Couples frequently report that intimacy shifts from a goal-oriented race to a broader sensory experience. Without the distraction of impending ejaculation, the entire encounter becomes elongated. Is it identical to your twenties? No, but many partners find the heightened vulnerability actually fosters a more profound psychological connection than before the diagnosis. The focus shifts entirely toward skin-to-skin resonance and deliberate, prolonged stimulation.
What role do non-surgical aids play in restoring a couple's sex life?
They act as a crucial bridge rather than a permanent crutch. Intracavernosal injections boast a success rate exceeding 70 percent, providing rigid erections regardless of nerve damage. Constriction rings and alprostadil suppositories offer alternative pathways for those wishing to avoid needles. These tools strip away the performance anxiety that frequently paralyzes a relationship after cancer treatment. By utilizing these medical assists early on, couples maintain their sexual routines instead of retreating into separate bedrooms out of sheer awkwardness.
A definitive verdict on pelvic intimacy
We need to stop treating the prostate as the sole custodian of male sexuality. Stripping away a cancerous gland does not hollow out a man's capacity for profound romantic resonance. The issue remains that societal scripting ties masculinity directly to fluid emission, an absurdly narrow definition of pleasure. True intimacy thrives on adaptive resilience, a willingness to rewrite the physical script when the old choreography fails. Medically speaking, can a man love without his prostate with fierce intensity? He can, and he should, because the heart and the brain remain the ultimate sex organs (and thankfully, no surgeon can resect those).