Decoding The Paradox: What Does An Abnormal Pap Smear But No HPV Co-Test Actually Mean?
For decades, the medical community treated every abnormal cervical scrape with identical panic. Then came the co-test. When a clinician evaluates your cervix today, they look at two distinct metrics: the physical shape of your cells via the Pap smear, and the presence of high-risk viral DNA via the HPV test. When you see an abnormal Pap smear but no HPV result on your portal, it means the cytologist found cells that do not look like textbook perfections, yet the biological engine that drives malignant transformation simply is not there.
The Statistical Reality of the Co-Test Discordance
You are not a medical anomaly. In fact, large-scale clinical data from the Kaiser Permanente Northern California screening cohort—which tracked over one million women—revealed that a significant percentage of abnormal cytology occurs in the absolute absence of HPV. Specifically, for patients presenting with Atypical Squamous Cells of Undetermined Significance, commonly known as ASC-US, up to fifty-five percent test negative for the virus. The thing is, our modern testing mechanisms are almost too sensitive. They catch microscopic cellular deviations that our bodies would normally fix over a weekend without us ever knowing.
Why the Medical System Separates Cell Shape From Viral Presence
Think of your cervix as a busy transit hub. The Pap test is a snapshot of the commuters' faces, while the HPV test checks for a specific bad actor at the gate. If the commuters look frazzled, is it because a villain is loose, or did the train just break down? Because ninety-nine point seven percent of cervical cancers are linked to high-risk HPV strains like HPV 16 and 18, a negative viral test acts as a massive safety net. Honestly, it is unclear why some clinical guidelines still trigger aggressive follow-ups for these low-risk scenarios, as many top gynecologists now argue that an HPV-negative abnormal smear is mostly clinical noise.
The True Culprits Behind Cervical Cellular Changes When HPV Is Absent
If the virus isn't causing trouble, what is? Your cervix is an incredibly sensitive mucous membrane, prone to reacting to the slightest environmental shift. It exists in a state of dynamic equilibrium, constantly shedding layers and defending itself against mundane daily stressors.
Benign Inflammation and the Vaginal Microbiome Chaos
The most frequent instigator of an abnormal Pap smear but no HPV is simple, unadulterated inflammation, clinically labeled as severe cervicitis. When your vaginal microbiome loses its dominant Lactobacillus population, opportunistic bugs move in. Conditions like Bacterial Vaginosis, or an overgrowth of Gardnerella vaginalis, alter the local pH drastically. This acidic volatility irritates the squamous epithelial cells. Yeast infections or common protozoan shifts like Trichomoniasis can cause cells to swell, change shape, and mimic precancerous distortions under a laboratory microscope. But we are far from actual malignancy here; it is just cellular irritation.
The Mechanical and Chemical Irritants Nobody Warns You About
People don't think about this enough: what did you do forty-eight hours before your annual exam? Recent sexual intercourse, the use of spermicides, or even residual lubricants from a pelvic ultrasound can cause physical micro-trauma to the delicate transformation zone of the cervix. The spatula or brush used during the collection process then picks up these bruised, regenerating cells. When the pathologist looks at them, the healing cells appear enlarged and hyperchromatic. Why? Because they are rapidly dividing to repair a minor scratch. Did you know that even a latex condom sensitivity can leave your cervical cells looking distorted enough to trigger a positive Pap flag?
Biological Milestones That Mimic Abnormal Cytology
Your birth certificate plays a massive role in how your cells behave under a microscope, making age-related biological transitions a prime suspect for confusing lab reports.
The Estrogen Drought and Atrophic Vaginitis
If you are perimenopausal, postmenopausal, or even breastfeeding, your estrogen levels are fluctuating or plummeting. Estrogen is what keeps the vaginal and cervical walls plush, thick, and well-lubricated. Without it, the tissue undergoes atrophy. The cells become small, parakeratotic, and dry. When a lab technician evaluates an atrophic smear from a woman in her fifties, differentiate between true dysplasia and simple hormone depletion becomes exceptionally difficult. It is a known diagnostic trap that frequently leads to an erroneous ASC-US diagnosis. A quick two-week course of localized estrogen cream usually clears this up, proving that the "abnormality" was just a lack of hormonal hydration.
Cervical Polyps and Benign Metaplasia
Another common factor is squamous metaplasia. This is a entirely normal, non-cancerous process where the fragile columnar cells of the inner cervical canal transform into tougher squamous cells to protect themselves. It is a biological remodeling project. However, during the active phase of this transition, the cells look highly irregular. Similarly, small, benign growths called cervical polyps—which affect roughly two to five percent of women—can shed atypical cells during a routine scrape. These cells look weird because they were scraped off a friable, vascular protrusion, not because they are mutating into something dangerous.
Navigating Your Lab Report: Deciphering the Fine Print
Understanding the vocabulary of your pathology report is paramount to regaining peace of mind, as different terms carry wildly different levels of clinical urgency.
| ASC-US | Negative | Mildly atypical cells, likely caused by irritation or infection. | Repeat co-test in 1 to 3 years. |
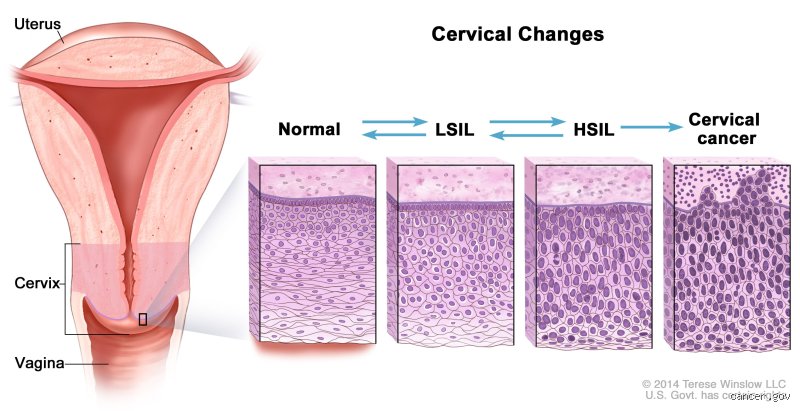
| Low-Grade SIL (LSIL) | Negative | Mild dysplasia present; highly unlikely to progress without the virus. | Repeat testing or occasional colposcopy based on age. |
| High-Grade SIL (HSIL) | Negative | Significant cellular changes; requires immediate closer inspection. | Colposcopy with biopsy to rule out rare false negatives. |
| Atypical Glandular Cells (AGC) | Negative | Cells from the inner canal look abnormal; demands careful evaluation. | Colposcopy, endocervical curettage, or endometrial sampling. |
When ASC-US and LSIL Clash With a Negative HPV Test
If your report reads ASC-US or LSIL alongside a negative HPV result, you can generally breathe a sigh of relief. The American Society for Colposcopy and Cervical Pathology, or ASCCP, updated their risk-based management consensus guidelines to explicitly state that the five-year risk of developing advanced cervical intraepithelial neoplasia grade three—known as CIN 3—in an individual with ASC-US and a negative HPV test is a mere zero point zero three percent. That changes everything. Yet, the issue remains that receiving an automated electronic medical record notification with the word "ABNORMAL" in bold red text causes immediate psychological distress, even when the actual risk is practically microscopic.
Common mistakes and misconceptions about Pap results
Equating an abnormal result with a cancer diagnosis
Panic is a reflex, yet it is entirely misplaced here. When a patient receives a notification stating their cervical screening requires attention, the mind immediately races toward oncological dread. Let's be clear: an atypical cellular reading is not a death sentence. The problem is that the public views the Papanicolaou test as a binary cancer detector. In reality, it functions as an early warning radar system, catching cellular deviations decades before they morph into malignancy. Statistics show that out of approximately 3 million abnormal cervical cytologies reported annually in the United States, less than 1% represent invasive carcinomas. The vast majority are minor, transient shifts that resolve without intervention.
Assuming a negative HPV test means zero cellular risk
Can a virus-free status give you a false sense of security? Absolutely. Many individuals discover a situation where a Pap smear abnormal but no HPV co-test exists, and they assume a laboratory error occurred. This is a dangerous miscalculation. Because human papillomavirus drives roughly 95% of cervical malignancies, we often forget the remaining 5% that bypass this viral pathway entirely. Believing you are entirely immune to cervical issues simply because your viral panel came back clean ignores the complex, non-viral etiologies that alter epithelial tissues. It creates a blind spot in gynecological health tracking, which explains why regular follow-ups remain vital regardless of your viral status.
Ignoring the impact of recent intercourse or hygiene products
The cervix is an incredibly sensitive anatomical structure. Chemical irritants found in spermicides, lubricants, or vaginal douching formulas can induce localized inflammation that look identical to dysplastic changes under a microscope. Furthermore, having sexual intercourse within 48 hours of your appointment can leave behind cellular debris or cause minor micro-trauma. As a result: the cytotechnologist encounters a field of distorted cells, leading to a false-positive reading. It is a frustratingly common scenario where mundane lifestyle variables trigger a terrifying medical notification.
The overlooked impact of severe estrogen depletion
How hormonal shifts mimic cervical dysplasia
There is a lesser-known biological phenomenon that frequently triggers these confounding lab results: atrophic vaginitis. As individuals transition into perimenopause and menopause, circulating estrogen levels plummet precipitously. This hormonal starvation causes the vaginal and cervical mucosa to thin out, lose elasticity, and become highly susceptible to inflammation. When the clinician scrapes these fragile tissues, the cells appear fragile, distorted, and possess enlarged nuclei due to the lack of hormonal support. Under the microscope, these benign, starved cells look deceptively similar to low-grade squamous intraepithelial lesions.
The estrogen challenge as a diagnostic strategy
When faced with an anomalous report in a patient over 50, savvy clinicians do not rush to perform invasive biopsies immediately. Instead, they utilize a brilliant diagnostic workaround known as the topical estrogen challenge. The issue remains that we often over-treat conditions that merely require a simple hormonal cream. By prescribing a short course of localized estrogen therapy for two to three weeks, we can revitalize the cervical tissue. If a subsequent smear comes back perfectly pristine, we know the previous abnormal Pap smear but negative HPV status was merely a reflection of tissue atrophy rather than true precancerous pathology. It is an elegant way to avoid unnecessary surgical interventions in menopausal patients.
Frequently Asked Questions
What is the statistical likelihood that an abnormal Pap without HPV indicates true precancer?
The probability is remarkably low, hovering around 2% to 5% for high-grade lesions in this specific demographic. Large-scale clinical trials tracking co-testing outcomes demonstrate that a concurrent negative viral screen provides a 99% negative predictive value against developing advanced cervical disease over the subsequent five years. Most of these anomalies stem from benign inflammation, severe tissue atrophy, or minor glandular irregularities. Consequently, standard medical guidelines generally recommend conservative management, such as repeating the co-test in 12 months, rather than rushing into immediate, aggressive surgical excisions.
Can a previous, cleared HPV infection cause permanent Pap alterations?
Yes, because the human immune system can successfully suppress or entirely eradicate the viral load while leaving behind minor, permanent structural scars within the cervical transition zone. Even though the modern polymerase chain reaction tests cannot detect the virus because it is no longer actively replicating, the subtle cellular changes remain visible to the cytologist. This historical viral activity mimics low-grade squamous abnormalities during routine screenings. Except that these structural changes are essentially biological footprints rather than an active, dangerous infection requiring immediate surgical ablation.
How does a clinician determine if an abnormal reading is a false positive?
The determination relies on a meticulous combination of clinical history tracking, symptom evaluation, and targeted visual inspection. If a patient presents with a history of severe vaginal dryness, recent chemical exposure, or pelvic radiation, the likelihood of a false positive skyrockets. Clinicians often use a colposcopy to visually inspect the cervix under high magnification using an acetic acid wash. When the visual field appears completely normal despite the concerning lab paperwork, the initial abnormal Pap smear but negative HPV results are officially deemed a benign false alarm caused by localized tissue irritation.
A definitive perspective on navigating confusing cervical screenings
The current medical paradigm relies heavily on automated algorithms, but these protocols frequently strip away the nuanced reality of human biology. Finding yourself with a Pap smear abnormal but no HPV can feel like an existential paradox designed to induce maximum anxiety. We must stop treating every minor cellular variance as an emergency that requires immediate, invasive tissue destruction. Over-screening and over-treating healthy individuals causes documented psychological trauma and physical harm to cervical integrity (which can complicate future pregnancies). We must champion a clinical approach that values patient patience over panicked intervention. Trust the statistical reality that a virus-free cervix is an overwhelmingly safe cervix. Let us demand that healthcare providers take a deep breath, look at the broader hormonal context, and choose watchful waiting over premature surgical enthusiasm.