Let's be completely honest here: sitting in that paper gown, feet in stirrups while someone inserts a cold piece of stainless steel into your vagina is nobody’s idea of a good Tuesday afternoon. It is uncomfortable, it feels invasive, and for many, it triggers intense anxiety. Yet, stepping away from the speculum entirely carries consequences that stretch far beyond a temporary moment of medical awkwardness.
The anatomy of neglect: understanding what a Pap smear actually hunts for
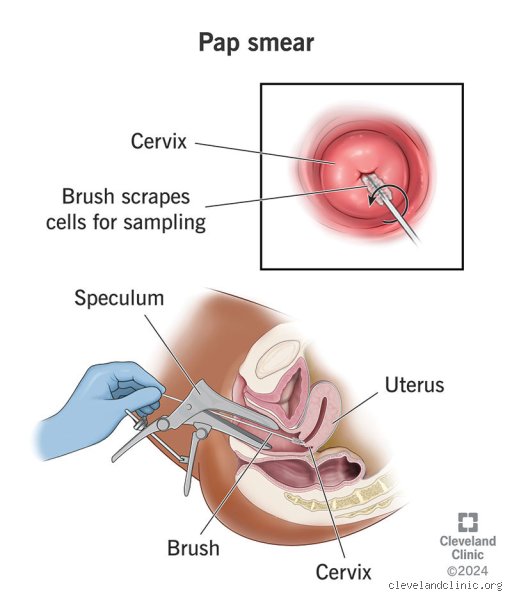
To understand the stakes, we have to look at what this test actually does, because a lot of people mistakenly think it searches for active cancer. It does not. A Pap smear is a cellular stakeout designed to catch abnormal changes—called dysplasia—long before they ever turn into a malignant tumor. During the procedure, a clinician gently scrapes the transformation zone of the cervix, which is the exact border where delicate endocervical columnar cells meet the tougher squamous cells of the vagina. This microscopic border town is precisely where human papillomavirus (HPV) likes to set up camp.
The viral squatter you probably already have
Here is a piece of data that usually shocks people: the Centers for Disease Control and Prevention (CDC) estimates that over 85% of sexually active adults will contract at least one type of HPV during their lifetime. It is the common cold of reproductive health. In most individuals, the immune system cleans up the virus within two years without you ever knowing it was there. But what happens if your body cannot clear it? That changes everything. When high-risk strains, specifically HPV 16 and 18, embed themselves into the cervical epithelial layer, they begin to slowly hijack the cellular replication machinery.
The slow-motion derailment of cervical cells
The progression from a healthy cell to a cancerous one is not an overnight mutation. It is a agonizingly slow journey that usually takes between 10 to 20 years, which explains why missing a single test rarely results in catastrophe, but skipping them forever is a completely different story. Pathologists categorize these changes as Cervical Intraepithelial Neoplasia, graded from CIN 1 (mild dysplasia) to CIN 3 (severe, carcinoma in situ). If you never get tested, you completely bypass the opportunity to catch the cells while they are still in the CIN 1 or CIN 2 stage, where a simple, minor outpatient procedure like a Loop Electrosurgical Excision Procedure (LEEP) could strip them away instantly.
The silent timeline: what happens inside your body over 20 years of screening absence
If you drop out of the screening pool entirely, your body is left to its own devices. What does that actually look like on a timeline? In the first five years of zero screening, assuming an oncogenic HPV strain has taken hold, cells in the transformation zone begin to lose their normal architecture. You will feel absolutely nothing. There is no pain, no unusual discharge, and your menstrual cycle will continue with its usual predictability. Why would you suspect anything is amiss? This is where it gets tricky, because the complete absence of symptoms convinces women that their reproductive tract is perfectly healthy.
The tipping point around year ten
By year ten, those unmonitored abnormal cells may have breached the basement membrane, turning into microinvasive carcinoma. And this is the exact moment where the medical community sometimes fractures into debate; honestly, it's unclear exactly which infections will aggressively progress and which ones will remain indolent forever, as every individual's immune microenvironment is completely unique. Yet, the issue remains that without a Pap test, you have no radar. I strongly believe that relying on luck in the absence of diagnostic data is a losing strategy. When the tumor finally grows large enough to ulcerate, symptoms finally burst through, usually manifesting as contact bleeding after intercourse or unusual spotting between periods. But because these symptoms can easily mimic benign issues like cervical polyps or hormonal fluctuations, many women delay seeing a doctor for another year or two.
The cost of a late-stage discovery
When diagnosis finally happens because of symptoms rather than a routine screening, the clinical picture is often grim. According to data from the National Cancer Institute, the 5-year relative survival rate for localized cervical cancer is an encouraging 92%. However, if the disease has managed to slip past the cervix into surrounding pelvic tissue or the lymph nodes before it is discovered, that survival statistic plummets down to around 59%. If it distant metastasizes to organs like the lungs or liver, the number drops to a brutal 19%. You are no longer looking at a quick, preventive office treatment; instead, you are facing radical hysterectomies, external beam radiation, and cisplatin-based chemotherapy regimens.
The shifting paradigm: why the test you are skipping might not even be a Pap smear anymore
The medical landscape does not stand still, and if you have been avoiding the clinic for a decade, the actual science of screening has evolved beneath your feet. The traditional Pap smear, invented by Dr. George Papanicolaou way back in the 1940s, is no longer the sole king of the castle. In fact, major medical bodies, including the American Cancer Society, updated their guidelines to favor primary HPV testing over the traditional cytology-based Pap smear for individuals aged 25 to 65.
Cytology versus molecular detection
Why the shift? A standard Pap smear looks at cellular morphology—essentially, a cytotechnologist peers through a microscope in a lab, perhaps in a large facility like Quest Diagnostics in New Jersey, looking for weirdly shaped cells. It has a notorious false-negative rate that hovers somewhere around 20% to 30%, meaning it can occasionally miss abnormalities. Primary HPV screening, on the other hand, uses molecular diagnostics to search for the actual DNA or RNA of the high-risk viral strains. It is vastly more sensitive. If the virus isn't there, your risk of developing cervical issues over the next five years is essentially zero, which is why screening intervals have safely expanded from three years to five years for many women.
Are there valid workarounds for the speculum-averse?
If your refusal to do a Pap smear stems from trauma, severe vaginismus, or cultural barriers, the absolute worst thing you can do is just shut the door on the medical system entirely. We are far from the days when the old-school pelvic exam was the only option on the table. Alternative avenues are opening up globally. For instance, in countries like Australia and Denmark, public health systems have successfully integrated HPV self-sampling kits into their national screening registries. These kits allow women to collect their own vaginal swab in the complete privacy of their own bathroom, completely bypassing the speculum and the clinician's gaze.
The limits of self-collection
Except that there is a catch. A self-swab can only tell you if high-risk HPV is present in your vaginal canal; it cannot tell you if those viral particles have actually started damaging your cervical architecture. As a result: if your self-test comes back positive for a high-risk strain, you still have to go into the clinic for a diagnostic reflex Pap smear or a colposcopy to see what the virus is actually doing. In short, self-testing is a fantastic gatekeeper, but it cannot completely eliminate the occasional need for traditional clinical evaluation.