Why People Avoid the Exam Room and What We Are Actually Testing For
The reluctance is completely valid, yet the pathology does not care about our discomfort. When we talk about cervical cancer screening, we are diving into a landscape deeply altered by the introduction of the Papanicolaou test in the 1940s by Dr. Georgios Papanikolaou. Before this clinical breakthrough, cervical malignancies were a leading cause of reproductive mortality among women in Western nations, but today, widespread screening has reduced incidence rates by more than 70% in developed healthcare systems. Yet, the issue remains that a massive chunk of the population avoids the stirrups altogether due to trauma, pain, or systemic medical gaslighting.
The Anatomy of a Cervical Swab and Cellular Transformation Zones
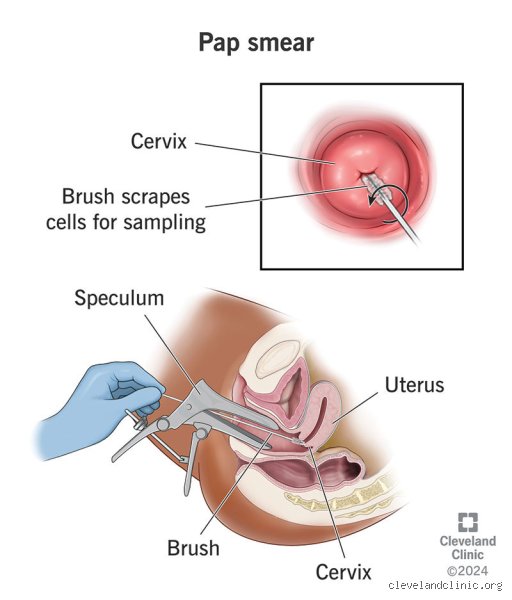
Where it gets tricky is understanding what the clinician is actually scraping. During a standard examination, cells are harvested from the transformation zone—the precise anatomical border where the delicate columnar epithelium of the endocervix meets the robust squamous epithelium of the ectocervix. Because this specific cellular zone undergoes constant remodeling (a natural process called squamous metaplasia), it is uniquely vulnerable to genetic mutations induced by viral pathogens. The scraped sample is smeared onto a glass slide or, more commonly now, suspended in a liquid-based cytology vial to look for dyskaryosis, which is just a fancy medical term for abnormal nuclear features. If you never get a Pap smear, these structural anomalies go entirely unnoticed, quietly replicating beneath the tissue surface over a timeline that can stretch across a decade.
[Image of cervical transformation zone]The Silent Catalyst: Unmasking the Human Papillomavirus
We cannot talk about skipping this test without addressing the literal elephant in the reproductive tract: the Human Papillomavirus (HPV). People don't think about this enough, but a staggering 80% of sexually active adults will contract at least one strain of this double-stranded DNA virus at some point in their lives. For the vast majority, a healthy immune system quietly clears the infection within 24 months without the individual ever knowing it existed. But when high-risk oncogenic strains persist, that changes everything.
The High-Risk Strains Pulling the Cellular Strings
There are over 200 recognized genotypes of this virus, yet a tiny, aggressive subset causes almost all cervical malignancies. Specifically, HPV 16 and HPV 18 are responsible for roughly 70% of all cervical carcinomas worldwide. These viral strains produce two highly problematic oncoproteins, known to pathologists as E6 and E7, which systematically dismantle our cells' natural tumor suppressor mechanisms—specifically targeting the p53 and retinoblastoma pathways. Imagine a car where someone has intentionally cut the brake lines; that is exactly what happens to cellular division when these viral proteins take over. And because this molecular sabotage happens entirely in the microscopic background, relying on "feeling healthy" is a completely useless metric for defense.
The Lengthy Timeline from Infection to Invasive Carcinoma
Here is the nuance that contradicts the frantic messaging you sometimes hear in clinic waiting rooms: cervical cancer does not develop overnight. The transition from a persistent viral infection to a high-grade squamous intraepithelial lesion (HSIL), and finally to invasive adenocarcinoma or squamous cell carcinoma, is an incredibly slow burn. It typically requires 10 to 20 years for these cellular deviations to break through the epithelial basement membrane. Except that in individuals with compromised immune systems—such as those living with poorly managed HIV or undergoing post-transplant immunosuppressive therapy—this defensive timeline collapses down to a mere 3 to 5 years. This varying latency period is precisely why missing a single test isn't an immediate death sentence, but completely abandoning the practice over a lifetime is an entirely different caliber of risk.
Quantifying the Danger: What Happens When Screening Disappears?
To truly grasp the stakes, we have to look at the bleak data from regions where preventive gynecology is virtually non-existent. According to historical data from registries in England and the Nordic countries, a individual who elects to completely bypass every single screening interval carries a significantly higher risk of presenting with late-stage, distant metastases. In these advanced scenarios, the five-year survival rate plummets dramatically compared to the 92% survival rate observed when the anomaly is caught while still localized to the cervix.
The Reality of Late-Stage Diagnoses in Underscreened Populations
I must emphasize that the vast majority of cervical cancers diagnosed today occur in individuals who have either never been screened or have not had a sample collected within the preceding five years. When a patient presents to an oncology ward in cities like Baltimore or Birmingham with breakthrough bleeding, pelvic pain, or renal failure caused by ureteral compression, the root cause is almost always an interrupted screening history. It is a frustrating, heartbreaking reality for clinicians because these tumors are inherently preventable. But is it ever acceptable to walk away from the testing schedule entirely? Well, experts disagree slightly on the exact age limits, but there is a very narrow demographic that can safely close the door on this specific medical chore without losing sleep.
Modern Alternatives and the Shift Toward Primary HPV DNA Testing
Thankfully, the medical landscape is evolving, and the classic cytology-based Pap smear is no longer the solitary king of the castle. In fact, major medical bodies, including the American Cancer Society, have shifted their primary recommendations toward standalone HPV DNA testing as the superior frontline defense. This method utilizes polymerase chain reaction (PCR) technology to detect the actual genetic material of the virus, offering a much higher sensitivity for identifying pre-cancerous lesions than looking at distorted cell shapes under a microscope.
The Rise of the At-Home Self-Sampling Kit
This molecular pivot has opened the floodgates for a massive logistical game-changer: self-sampling kits. For anyone who has avoided the clinic due to vaginismus, cultural barriers, or severe anxiety, this alternative changes the entire equation by allowing you to collect your own vaginal swab in the absolute privacy of your bathroom. You spin a small cotton swab, seal it in a biohazard tube, mail it to a molecular diagnostics lab, and receive a definitive readout on whether those high-risk viral strains are lurking in your system. This strategy is already widely integrated into public health infrastructure across Australia and the Netherlands, proving that while skipping cervical screening entirely is a massive gamble, we are far from the days when enduring a cold, metallic clinical exam was your only option for survival.
The Fatal Assumptions: Myths That Keep Exam Rooms Empty
Believing that a lack of sexual activity equals a zero-percent chance of oncogenic cellular mutations is a trap. Human Papillomavirus remains incredibly stubborn, often lurking dormant within epithelial tissue for decades before trigger factors cause it to misbehave. The problem is that many individuals assume a decade of celibacy grants them a lifetime pass from gynecological screening. It does not. Viruses do not follow our moral or relationship timelines, meaning an infection acquired in the nineties can suddenly manifest as pre-cancerous lesions today.
The "I Am Vaccinated" Shield
Receiving the Gardasil series during adolescence provides stellar protection against the most aggressive viral strains, yet it does not cover every single high-risk variant in existence. Do you really want to gamble your pelvic health on a partial shield? Relying solely on past inoculations creates a false sense of absolute security. The vaccine reduces your risk profile dramatically, but skipping your routine diagnostic evaluations entirely because of it remains a massive gamble.
Ageist Assumptions in Post-Menopausal Care
Another widespread delusion dictates that once the ovaries retire, the cervix becomes immune to malignancy. Except that cellular degradation cares very little about your reproductive status. Cervical cancer incidence rates spike significantly in older demographics who abandon regular screening protocols prematurely. Medical guidelines explicitly state testing should continue until at least age 65, provided prior results were consistently pristine.
The Stealth Factor: What Your Body Is Secretly Hiding
Cervical dysplasia is a ghost; it rarely makes a sound. By the time noticeable indicators like post-coital bleeding, pelvic pain, or atypical discharge surface, the pathological timeline has already advanced into dangerous territory. Let's be clear: waiting for physical symptoms to appear before booking an appointment completely defeats the purpose of preventive medicine.
The Co-Testing Paradigm Shift
Modern diagnostics have evolved far beyond the simple cellular scrape of yesteryear. Combining cytological evaluation with high-risk HPV DNA typing offers a dual-layered defense mechanism that identifies viral activity at the molecular level before structural cellular damage even begins. This dual approach increases diagnostic sensitivity exponentially, which explains why the traditional annual schedule has safely stretched to a five-year interval for many low-risk patients. If you choose a path where you never get a Pap smear, you completely lock yourself out of these highly sophisticated, preventative screening technologies.
Frequently Asked Questions
Is it okay if I never get a Pap smear if I have only had one sexual partner?
Monogamy reduces your exposure metrics significantly, but it does not completely eliminate the necessity for routine clinical surveillance. Research demonstrates that approximately 80 percent of sexually active adults will contract at least one strain of Human Papillomavirus at some point during their lifetimes, often from their very first encounter. A partner might harbor a completely asymptomatic, latent viral load for years without knowing it, which then gets transmitted effortlessly despite a completely exclusive relationship dynamic. Consequently, relying on a partner's perceived viral status as a primary defense strategy is highly reckless. Skipping diagnostic screenings entirely based on relationship longevity overlooks basic viral mechanics and leaves your long-term cellular health completely unprotected.
Can lifestyle modifications or diet substitute for clinical cervical screening?
An optimal diet rich in cruciferous vegetables, regular exercise, and avoiding tobacco products undeniably strengthens your systemic immune response, helping the body clear transient infections more efficiently. (Smoking, for example, doubles your risk of cervical progression because it depletes the specific immune cells within local cervical tissues). But no amount of kale, vitamins, or holistic lifestyle alterations can mechanically identify or reverse established pre-cancerous genetic mutations within the epithelium. When structural cellular changes trigger, they require precise localized medical monitoring or surgical intervention to stop them from crossing the basement membrane into invasive malignancy. Substituting wellness trends for verified cytological tracking is an inherently flawed strategy that offers zero diagnostic validity.
At what specific age is it genuinely safe to stop undergoing these procedures entirely?
The vast majority of major gynecological task forces agree that individuals can safely cease screening at age 65, but this liberation is strictly conditional. You must possess a documented history of three consecutive negative Pap results or two consecutive negative co-tests within the preceding ten years to earn this exit ticket. Anyone with a history of high-grade dysplasia remains under surveillance for at least twenty years following that specific diagnosis, regardless of their current age. Furthermore, individuals who underwent a total hysterectomy involving cervix removal for non-cancerous conditions can usually stop altogether, provided they have no prior history of severe neoplasia. As a result: unless you meet these highly specific, medically documented criteria, unilaterally abandoning the exam table remains highly ill-advised.
A Definitive Verdict on Avoiding the Speculum
Choosing a lifetime of total avoidance regarding cervical screening is not an act of bodily autonomy; it is an exercise in profound medical vulnerability. We must acknowledge the systemic failures, personal traumas, and intense physical discomforts that drive individuals to avoid the clinic entirely. Yet, ignoring a highly preventable malignancy because the diagnostic process feels invasive will never change the harsh biological reality of oncogenesis. The statistics do not lie, as roughly 4,000 women succumb annually to this specific disease in the United States alone, with the vast majority of those fatalities occurring in individuals who skipped their routine screenings. Refusing these simple cellular checks means voluntarily opting into a high-stakes lottery where the prize is a completely avoidable cancer diagnosis. It is time to prioritize survival over discomfort and stop pretending that avoiding the exam table carries no consequence. Take control of your health reality by advocating for better numbing options, trauma-informed practitioners, or self-collection alternatives rather than completely walking away from lifesaving diagnostics.