The Cellular Twilight Zone: Deconstructing Co-Testing Results
For decades, the annual Pap smear was the undisputed king of cervical screening. We stripped down, slid to the edge of the table, and endured the cold click of the speculum while doctors scraped away a few cells to peer at under a microscope. Simple. But in 2012, the U.S. Preventive Services Task Force shifted the paradigm by heavily endorsing co-testing—running a Pap and an HPV DNA test simultaneously for women aged 30 to 65. Why? Because looking at cells alone leaves too much to chance.
The Pap Smear Looks at Current Damage
Think of a Pap test as a structural inspection of a house. The cytologist at the lab is literally checking the architecture of your cervical cells to see if they look distorted, wild, or dysplastic. If the Pap is normal, the building is structurally sound today. But here is where it gets tricky: a normal Pap only tells us about the present moment, completely ignoring the invisible termite infestation that might be starting in the foundation.
The HPV Test Predicts Future Risk
That invisible threat is the virus itself. The HPV test doesn't care what the cells look like; it hunts for viral DNA. When you test positive, it means one of the 14 high-risk HPV strains, most notably HPV 16 or HPV 18, is hanging out in your epithelial tissue. I find the rigid clinical obsession with treating every positive HPV test as an impending catastrophe deeply flawed. The virus is incredibly common—the Centers for Disease Control and Prevention (CDC) notes that over 80 percent of sexually active adults will contract at least one strain of HPV in their lifetime. You might have caught it last month in Chicago, or it could have been slumbering quietly in your system since a college romance in Miami back in 2018. Honestly, it's unclear exactly when transmission occurs in most stable relationships, and honestly, tracking the origin is a fool's errand.
The Biology of a Stalemate: Why Normal Cells Coexist with a Active Virus
How can a virus be present without causing damage? It comes down to a biological Mexican standoff. Your immune system is an incredibly potent weapon, and most of the time, it keeps the virus tightly suppressed in a latent state where it cannot replicate enough to distort your cervical architecture. Yet, the virus is still detectable by highly sensitive molecular assays like the Cobas HPV test, which can pick up mere fragments of viral genetic material.
The Disconnect Between Infection and Transformation
An HPV infection is not a cancer diagnosis. We are far from it. For the vast majority of women, the immune system completely clears—or suppresses to undetectable levels—the virus within 12 to 24 months. The problem only arises when the infection becomes persistent. When a high-risk strain sets up a permanent camp over many years, it slowly begins to insert its own oncogenes, specifically E6 and E7, into the host cell DNA. This disruption flips a genetic switch, turning off the cell's natural suicide mechanism. But remember, this microscopic transformation takes a long time. We are talking about a timeline that typically spans 10 to 20 years from initial infection to actual cervical malignancy, which explains why a positive test alongside a normal Pap is an invitation for watchful waiting, not surgical intervention.
When the Immune System Takes a Temporary Nap
People don't think about this enough, but our immune surveillance fluctuates wildly based on lifestyle and stress. Did you recently go through a grueling divorce, pull consecutive all-nighters for a corporate merger, or battle a severe bout of influenza? A temporary dip in your cellular immunity can allow a long-dormant HPV infection to wake up and replicate just enough to trigger a positive result on a screening test, even though your cervical cells haven't had the time or the viral load exposure to become damaged. That changes everything regarding how we interpret a single isolated positive result.
The Clinical Crossroads: What Happens Next in the Doctor's Office?
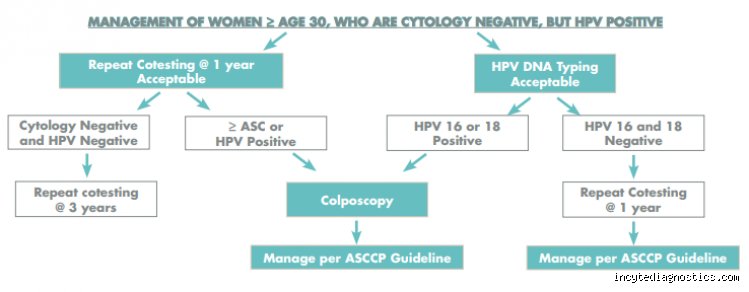
So you have this specific combination of results. What does your gynecologist actually do with you? They don't just guess. Instead, they turn to the rigorous, algorithm-driven guidelines established by the American Society for Colposcopy and Cervical Pathology (ASCCP).
The Standard Protocols for Mixed Screening Profiles
The management path depends heavily on your age and your specific screening history. If you are 30 or older and this is your very first time testing positive for HPV with a normal Pap, the standard recommendation is usually to repeat the co-test in exactly 12 months. This waiting period gives your immune system a fair chance to clear the viral load naturally. Except that if the specific strain identified happens to be HPV 16 or HPV 18—the two aggressive genotypes responsible for roughly 70 percent of all cervical cancers worldwide—the doctor will bypass the waiting game entirely and recommend a colposcopy immediately, regardless of how pristine your Pap looks.
The Psychological Toll of Watchful Waiting
This is where the medical guidelines clash brutally with human psychology. Telling a patient they have a cancer-associated virus but instructing them to go home and worry about it for a year is an agonizing clinical strategy. Is it scientifically sound? Absolutely. But the emotional anxiety it creates is immense. Patients frequently spiral, assuming that a ticking time bomb has been planted inside their reproductive tract, which often leads to frantic demands for aggressive, unnecessary procedures like LEEP or biopsies that can permanently scar the cervix.
Sifting Through the Options: Primary HPV Testing vs. Traditional Co-Testing
The medical community is currently locked in a fierce, nuanced debate over the best way to handle cervical cancer screenings moving forward, and experts disagree on whether the Pap smear should even remain part of the initial conversation.
The Rise of Primary HPV Screening
Many major health organizations, including the American Cancer Society, are pushing hard to replace co-testing altogether with Primary HPV screening starting at age 25. Under this protocol, you only get a Pap smear if your initial HPV test comes back positive first. The argument is that the HPV test is vastly more sensitive than the Pap, making the traditional cellular scrape redundant as a frontline tool. As a result: we are seeing a massive shift in lab logistics globally, from London to Sydney, as pathology departments phase out old-school cytology in favor of automated molecular platforms.
Why Some Clinicians Resolutely Cling to the Pap Smear
But the issue remains that primary HPV screening throws a incredibly wide net, catching millions of transient, harmless infections that would have vanished on their own without ever causing a single abnormal cell. The Pap smear acts as a vital quality control filter. By looking at the physical cells, clinicians can successfully separate the patients who need immediate medical eyes on their cervix from the patients who simply have a quiet, lazy viral infection that needs nothing more than time. In short, losing the Pap completely might lead to an epidemic of over-treatment, proving that older diagnostic tools still hold immense value in a high-tech world.
Common mistakes and misconceptions about discordant screening results
Receiving news that your Pap is normal but HPV is positive often triggers immediate, unnecessary panic. The primary blunder patients commit is equating a positive viral screen with an active cancer diagnosis. It is nothing of the sort. Let's be clear: the virus is merely an unwelcome hitchhiker, not a malignant tumor. Because the human papillomavirus operates quietly in the background, a normal Pap smear simply indicates that your cervical cells currently show zero architectural distortions. The system is working exactly as intended by catching the risk factor long before any actual cellular damage manifests.
The timeline fallacy and the blame game
Another frequent trap is assuming a positive viral test implies recent infidelity. This microscopic pathogen is notoriously patient. It can linger in a somnolent state within your epithelial tissues for decades, flying completely under the radar. Suddenly, perhaps due to a transient dip in your immune surveillance, it awakens. You cannot use this diagnostic result to reconstruct a timeline of your past relationships, nor should you. Trying to pinpoint the exact moment of transmission is an exercise in futility, except that it causes needless relationship friction.
Overtreatment anxiety and the rush for procedures
Many individuals demand aggressive interventions the moment they see a positive result. They want the virus cut out, burned away, or eradicated immediately. Medical science possesses no magic pill to cure the viral infection itself. Eradication is a task solely reserved for your own immune defenses. Rushing into invasive cervical procedures when your Pap is normal but HPV is positive is actually counterproductive. Unnecessary surgical interventions on a healthy cervix can weaken the tissue, which explains why guidelines heavily favor watchful waiting over immediate scalpel work.
The hidden micro-environment: Immune health and viral clearance
While standard medical literature focuses intensely on the viral genotype, the intricate choreography of your vaginal microbiome receives far less spotlight. The localized ecosystem of bacteria playing out inside you dictates whether the virus packs its bags or settles in for a long stay. A diverse, Lactobacillus-dominated environment acts as a biological shield, keeping viral replication tightly suppressed.
Nurturing your cellular defense network
How do we tip the scales back in our favor? Chronic psychological stress releases sustained bursts of cortisol, a hormone known to dull your immune response. When cortisol dampens your natural killer cell activity, the virus seizes the opportunity to persist. Focusing on sleep optimization, smoking cessation, and targeted nutritional support creates a hostile environment for the pathogen. In short, your daily lifestyle choices directly influence whether your body successfully clears the infection or allows it to linger until the next annual checkup.
Frequently Asked Questions
Can I still pass the virus to my partner if my Pap is normal but HPV is positive?
Yes, transmission remains highly probable because the virus resides on the surface of the skin and mucosal membranes, irrespective of what your cervical cells look like under a microscope. Data from global epidemiological studies demonstrate that approximately 80 percent of sexually active adults will acquire at least one strain of this virus at some point in their lives. Condoms offer excellent barriers against many pathogens, yet they only reduce the transmission risk of this specific virus by about 70 percent because they do not cover every square inch of pelvic skin. The issue remains that your current partner has likely already been exposed to the virus, making frantic prophylactic changes at this stage largely redundant. Consequently, barrier methods are excellent for general hygiene, but they are not an absolute guarantee against viral sharing.
How long does it typically take for the immune system to clear the infection?
The vast majority of young, healthy individuals will successfully suppress the viral invader without any medical assistance. Clinical data indicates that roughly 90 percent of viral infections become undetectable within a strict window of 12 to 24 months. Your body deploys specialized T-cells to neutralize the viral particles, a process that usually leaves no permanent scars or cellular traces behind. What if your follow-up test next year still shows the virus is active? A persistent infection over multiple years is the specific scenario that requires closer clinical scrutiny, which is why doctors mandate a repeat co-testing kit after twelve months rather than letting you skip your checkups entirely.
Does a positive test mean I will definitely need a colposcopy?
Not necessarily, as the management pathway depends heavily on your age and the specific viral strain identified. If your screening panel reveals the presence of high-risk genotypes like HPV 16 or 18, guidelines often dictate an immediate referral for a colposcopy, even with a completely pristine Pap history, because these two strains account for roughly 70 percent of cervical malignancies globally. For other, less aggressive high-risk strains, the standard medical protocol recommends simply repeating the co-test in one year. Why undergo invasive visual testing when your cellular structure is currently pristine? Statistics show that a massive chunk of these transient infections resolve spontaneously during that twelve-month waiting period, saving you from unnecessary emotional distress and uncomfortable pelvic exams.
A definitive stance on modern cervical screening
We need to stop viewing a positive viral screen as a ticking time bomb and start recognizing it as the ultimate preventative luxury. Decades ago, medicine could only react once full-blown malignant cells had already ravaged the cervix. Today, knowing your Pap is normal but HPV is positive grants you a massive head start, a literal window of years to monitor and support your body before an illness even dreams of developing. It is a profound triumph of predictive analytics over reactive crisis management. Do not let diagnostic anxiety overshadow the reality that you are remarkably safe, thoroughly monitored, and fully in control of your reproductive health. Demand clear strain identification from your clinician, protect your immune system fiercely, and view the situation not as a medical crisis, but as an early warning system operating in absolute perfection.