The Hidden Architecture of Blood Flow: What MAP Actually Tells Us
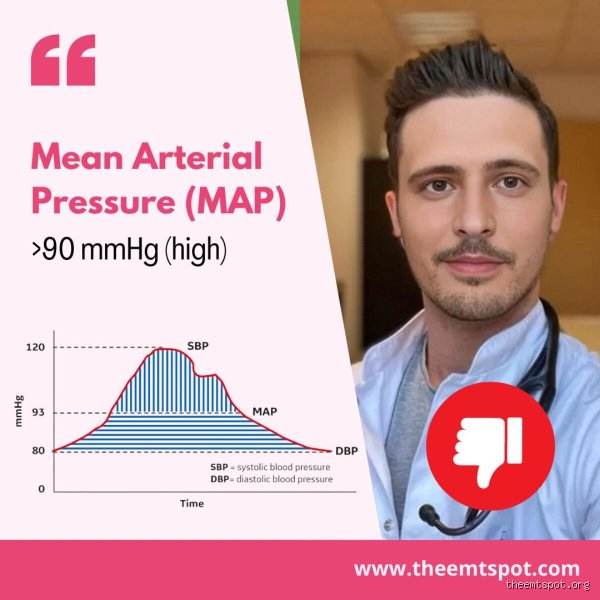
We are obsessed with the two standard numbers, the systolic and diastolic pressures, yet the body experiences blood flow as a continuous, dynamic wave. This is where Mean Arterial Pressure steps in. It is not a simple average of those two numbers because the heart spends twice as much time relaxing in the diastolic phase as it does contracting during systole. Think of it like a plumbing network in an old municipal building; the peak surges matter, but the constant, baseline stress against the pipe walls determines when a leak will finally burst. When you calculate this value, a normal, healthy baseline sits comfortably between 70 and 100 mmHg to keep everything running smoothly.
The Math and the Myth Behind the Formula
How do we actually arrive at this number? The math relies on a specific ratio: you take the diastolic pressure, double it, add the systolic pressure, and then divide that entire sum by three. For example, if a patient presents at a clinic in Chicago with a reading of 140/95 mmHg, the calculation yields a MAP of precisely 110 mmHg. Where it gets tricky is assuming that everyone with this score shares the same cardiovascular reality. A young athlete experiencing acute stress might spike to this level temporarily, whereas an older sedentary individual might permanently reside there, which changes everything regarding long-term organ damage.
Perfusion Versus Pressure: The Delicate Internal Balance
Your organs require a minimum pressure gradient to force oxygenated blood through tiny, microscopic capillary beds. If the MAP drops below 60 mmHg, vital organs like the kidneys and brain starve, a catastrophic state known as hypoperfusion. But flip that script. When the pressure climbs to a MAP of 110, the delicate endothelial lining of your blood vessels faces a relentless, abrasive pounding. It is a paradox because the body needs pressure to survive, yet that very same force, when left unchecked, gradually destroys the microvasculature of the brain and kidneys.
Why a MAP of 110 Is Too High: The Physiological Toll on Organs
Living with a MAP of 110 mmHg means your heart muscle is constantly pushing against an invisible, stubborn wall of resistance. This resistance forces the left ventricle to thicken and hypertrophy over time, a structural change that sounds protective but actually makes the heart stiff and inefficient. The situation worsens when you look at the delicate filtration systems in the human body. The kidneys, specifically the tiny clusters of capillaries known as glomeruli, are designed to filter waste under precise, regulated pressures. Bombarding them with a perpetual MAP of 110 is akin to power-washing a delicate silk curtain; eventually, the fabric frays, leading to chronic renal insufficiency.
The Neurological Threat: White Matter and Silent Strokes
The brain does not tolerate pressure volatility well. While cerebral autoregulation protects the brain across a wide range of pressures, a sustained MAP of 110 pushes the upper limits of this protective mechanism. Over months and years, this relentless pressure compromises the blood-brain barrier, causing microvascular damage that neurologists frequently identify on MRI scans as white matter hyperintensities. People don't think about this enough, but this silent, asymptomatic vascular wear-and-tear is a leading driver of vascular dementia. Are you willing to ignore a number that actively erodes cognitive reserve? The issue remains that because you cannot feel your MAP, the damage accumulates in total silence until a major clinical event occurs.
Endothelial Dysfunction: When the Arteries Lose Their Flexibility
Healthy blood vessels resemble supple, elastic bands that expand and contract effortlessly with every single heartbeat. Chronic exposure to elevated pressures disrupts the production of nitric oxide, a vital molecule responsible for keeping these vessels dilated. As a result: the smooth muscle cells within the arterial walls thicken, turning those once-flexible tubes into rigid, scarred conduits. This rigidity creates a dangerous feedback loop where increased stiffness drives the pressure even higher, accelerating the progression of systemic atherosclerosis throughout the entire body.
Clinical Context: When 110 Is an Emergency Versus a Temporary Spike
Context dictates the urgency of a MAP of 110 mmHg. If a nurse records this number while you are sitting quietly in a calm examination room, it points toward established Stage 2 hypertension that requires medical intervention. However, if this reading occurs during an intense workout or right after a massive dose of caffeine, it might just be a transient physiological spike. The human body is designed to handle temporary surges. Honestly, it's unclear to many patients where the line between a normal reaction and a chronic pathology lies, which is why a single isolated reading should never be used to diagnose a lifelong cardiovascular condition.
White Coat Hypertension and the Anxiety Factor
The sheer stress of walking into a sterile medical facility can cause a patient's blood pressure to skyrocket instantly. A well-documented 2019 study published in the Journal of the American Medical Association revealed that up to twenty percent of patients exhibit significantly higher readings in clinical settings compared to their home environments. This phenomenon, widely known as white coat hypertension, can easily push a patient's resting MAP from a benign 95 up to a concerning 110 mmHg. To counter this, physicians now rely heavily on ambulatory blood pressure monitoring, which tracks numbers over a full twenty-four-hour cycle to capture a realistic snapshot of daily life.
Acute Stress Factors in the Emergency Department
In emergency medicine, a MAP of 110 is a frequent finding during acute crises. Pain, severe anxiety, alcohol withdrawal, or acute urinary retention can send the sympathetic nervous system into overdrive, flooding the bloodstream with epinephrine and norepinephrine. In these high-stakes scenarios, treating the underlying cause, such as administering appropriate pain relief, often brings the pressure back down to a safe baseline without the use of dedicated antihypertensive medications. Except that if the patient also exhibits signs of target organ damage, such as chest pain or neurological deficits, that same 110 MAP suddenly becomes a harbinger of a hypertensive emergency.
Comparing MAP to Traditional Readings: Why This Metric Matters More
Traditional blood pressure readings offer two distinct data points, but they fail to convey the continuous workload placed on the vascular tree. A reading of 160/85 mmHg and a reading of 130/100 mmHg look entirely different on paper, yet both generate a MAP of approximately 110 mmHg. That changes everything for a clinician trying to assess risk. The patient with the high diastolic pressure faces a constant, unyielding baseline stress, whereas the patient with the high systolic reading experiences sharper, more violent pressure waves. By looking at the MAP, we unify these different presentations into a single, highly predictive metric of cardiovascular strain.
The Critical Limitations of Isolated Systolic Tracking
Focusing exclusively on the top number can lead to dangerous clinical blind spots, particularly in middle-aged adults. Someone might shrug off a systolic reading of 135 mmHg, assuming they are hovering just above normal, but if their diastolic pressure is stuck at 98 mmHg, their MAP is sitting at a dangerous 110 mmHg. We are far from a comprehensive understanding of cardiovascular health if we only glance at the first number on the monitor. The continuous, mean pressure is what actually dictates the shear stress experienced by the endothelial walls on a minute-by-minute basis.
Predictive Value in Intensive Care and Anesthesia
Inside the intensive care unit, doctors rarely look at the traditional blood pressure fraction; they monitor the MAP continuously via arterial lines. During major surgeries, maintaining a stable MAP is the primary goal for the anesthesia team to ensure that the patient's brain and kidneys receive adequate blood flow throughout the procedure. While a MAP of 110 is generally avoided because it increases bleeding risks at the surgical site, it provides a much more stable, real-time indicator of systemic perfusion than fluctuating systolic peaks, which explains why it remains the gold standard metric in critical care medicine across the globe.
Common mistakes and misconceptions about mean arterial pressure
The single-reading panic trap
You stare at the monitor. The digits flash. A MAP of 110 glares back at you, triggering immediate medical anxiety. The problem is that a solitary metric represents nothing more than a fleeting physiological snapshot. Human vasculature behaves like a dynamic accordion, expanding and contracting based on stress, caffeine, or an uncomfortably full bladder. Clinicians frequently witness patients obsessing over one elevated number. But is a MAP of 110 too high when you have just sprinted up three flights of stairs? Absolutely not. True clinical significance emerges only when we look at sustained trends over several hours, except that anxious patients rarely want to wait for a trend line to develop.
Confusing MAP with systolic pressure
Let's be clear: mean arterial pressure is not simply the average of your top and bottom blood pressure numbers. Many individuals mistakenly add the systolic and diastolic numbers together and divide by two. This mathematical shortcut is fundamentally wrong because the heart spends twice as much time resting in diastole as it does contracting in systole. To calculate the actual perfusion pressure, we must use a specific formula where we double the diastolic reading, add the systolic, and then divide by three. A systolic reading of 110 mmHg is perfectly healthy, which explains why people panic when they see a mean arterial pressure of 110 and assume it indicates the exact same physiological state.
Ignoring the context of the patient
Context changes everything in medicine. For a young, healthy athlete, a mean arterial pressure of 110 mmHg during a routine physical exam demands immediate investigation. Yet, the issue remains entirely different inside a neuro-intensive care unit. In patients suffering from acute ischemic stroke, cerebral perfusion pressures must be kept deliberately elevated to force oxygenated blood past blood clots into dying brain tissue. Lowering that number out of a misplaced desire for textbook perfection could actually induce a massive cerebral infarction. We must always treat the specific human being sitting on the examination table rather than mindlessly chasing an arbitrary, idealized numerical target on a digital screen.
The hidden danger of arterial stiffness and expert advice
The stealthy toll on microvasculature
While a temporary spike in pressure is harmless, a chronic MAP value over 100 mmHg acts like a high-pressure power washer inside delicate plumbing. Over time, this relentless hydraulic pounding shears away the microscopic endothelial lining of your blood vessels. Because the body attempts to repair this structural damage by laying down rigid scar tissue, the arteries lose their natural elasticity. This creates a dangerous, self-reinforcing feedback loop. As the arterial walls stiffen, the heart must pump even harder to move blood, pushing the baseline pressure higher. Did you know that your tiniest capillaries in the kidneys and retinas are the very first casualties of this silent mechanical warfare?
How to properly validate your perfusion data
If you are tracking your metrics at home, precision is everything. Sit quietly in a supportive chair with your feet flat on the floor for a full five minutes before pressing the start button on your automated cuff. Keep your arm elevated exactly at the level of your heart, as positioning it too low will artificially inflate your numbers. Experts recommend taking three distinct readings separated by two minutes, throwing out the first result entirely, and averaging the final two. This rigorous method eliminates the adrenaline-fueled artifact known as white-coat hypertension, ensuring your doctor receives clean, actionable data to make informed therapeutic decisions.
Frequently Asked Questions
Is a MAP of 110 too high during intense physical exercise?
No, a MAP of 110 is completely normal and expected when your body is under heavy physical exertion. During strenuous workouts, your cardiac output skyrockets to deliver oxygen to straining skeletal muscles, which naturally elevates systemic pressures. Scientific data shows that a healthy athlete's mean arterial pressure can safely climb to 125 mmHg or higher during peak anaerobic performance without causing any cardiovascular damage. This acute elevation is entirely temporary, and your vascular system should return to its baseline resting state of 70 to 100 mmHg within thirty minutes of stopping the activity. As a result: you should never measure your baseline cardiovascular health immediately after lifting weights or running.
Can acute emotional stress cause your MAP to hit 110?
Yes, intense psychological stress or sudden panic attacks can rapidly drive your perfusion metrics into this elevated territory. When the sympathetic nervous system senses danger, it unleashes a massive flood of adrenaline and cortisol directly into your bloodstream. These powerful hormones cause your heart rate to spike and your peripheral blood vessels to constrict instantly. Clinical studies indicate that acute panic can cause an immediate 20% surge in overall mean arterial pressure. Once the psychological trigger is removed and your breathing slows down, your parasympathetic nervous system takes over to restore equilibrium. In short, a high reading during a stressful moment reflects a normal fight-or-flight response rather than chronic cardiovascular disease.
What symptoms usually accompany a sustained MAP of 110?
In the vast majority of cases, a chronically elevated perfusion pressure produces absolutely no physical symptoms at all. Hypertension has earned the ominous nickname of the silent killer because people can walk around for decades with dangerously high pressures while feeling completely healthy. However, when the metric spikes rapidly or stays sustained at extreme levels, individuals might experience throbbing occipital headaches, blurry vision, or a unexplained ringing in their ears. (A few patients also report a strange, pulsing sensation in their neck or chest during moments of quiet rest). Because you cannot rely on physical sensations to warn you of danger, regular objective monitoring remains the only reliable way to catch this hidden vascular strain.
A definitive medical stance on elevated perfusion
We cannot afford to be complacent about a sustained MAP of 110 because it represents a clear, unmistakable warning sign from the cardiovascular system. While an isolated high reading is no reason to rush to the emergency room, ignoring a consistent trend of elevated perfusion pressure is a recipe for long-term organ damage. This specific level of hydrostatic pressure forces the left ventricle of the heart to work unnecessarily hard, inevitably leading to myocardial hypertrophy and eventual heart failure. Modern medicine possesses an array of highly effective lifestyle interventions and pharmacological tools to gently guide these numbers back into a safe, optimal zone. You must take control of your vascular health by partnering with a qualified physician to investigate the root cause of this elevated pressure before it inflicts irreversible structural damage. Ultimately, acknowledging our physiological limits and taking proactive steps is the only way to guarantee long-term survival in an stressful world.