The Post-Menopause Shift: Why Your Lipid Profile Changed Completely After 50
For decades, your body operated under a distinct cardiovascular shield. Estrogen does a phenomenal job of keeping high-density lipoprotein levels elevated while keeping the less desirable fats in check, acting as a natural defense mechanism against arterial plaque buildup. Then, menopause hits. The subsequent hormonal cliff drops estrogen production significantly, which explains the sudden, often jarring spike in circulating blood lipids that women notice during their annual physicals in their late fifties and sixties. It is not necessarily a reflection of a sudden dietary failure or a sedentary lifestyle; it is basic biological restructuring.
The Estrogen Exit and the Sudden Surge in Circulating Lipids
When ovarian function winds down, the liver undergoes a quiet revolution in how it processes fats. Receptors that previously cleared low-density lipoprotein from your bloodstream become less efficient, meaning those particles circulate longer and have a higher probability of oxidizing. I find it deeply frustrating how often clinicians hand out generic lifestyle lectures to sixty-year-old women whose numbers jumped thirty points in a year, completely ignoring the fact that their endocrine system just underwent a massive, permanent rewrite. The thing is, this hormonal shift can alter your total lipid concentration by up to 15% to 20% without you changing a single thing about your breakfast routine.
Why Comparing Your Numbers to Men of the Same Age is a Dangerous Mistake
Historically, clinical cardiology treated women as smaller versions of men, a flawed methodology that led to decades of misdiagnosis. A man who has carried high total cholesterol since his thirties has a completely different arterial risk profile than a 64-year-old woman whose levels only rose after her final menstrual period. The male cardiovascular trajectory is often a slow, steady accumulation of plaque over forty years, whereas female risk often stays low and then accelerates sharply post-menopause. Because of this distinct timeline, applying identical treatment thresholds to both sexes is not just lazy medicine—it actively harms patients by either over-medicating low-risk women or ignoring unique female danger signs like microvascular dysfunction.
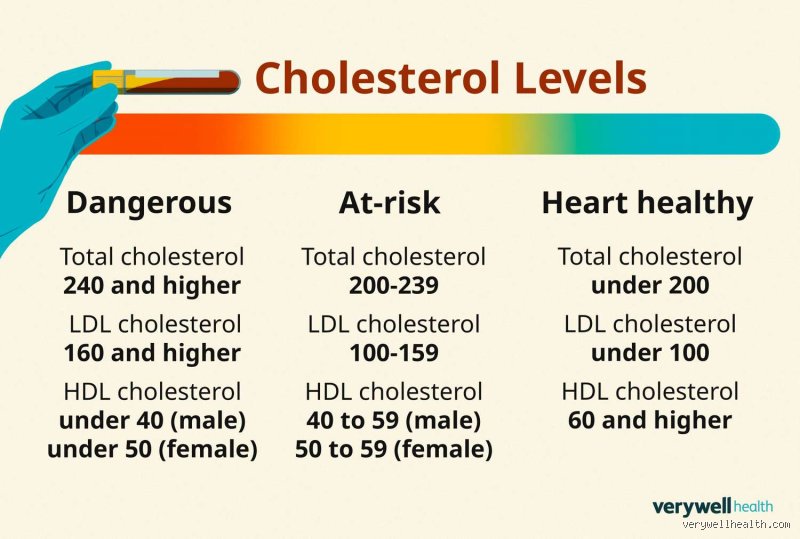
Decoding the Numbers: What Constitutes a Normal Cholesterol Level for a Woman Over 60?
Let us break down the specific components of a modern lipid panel because looking at total cholesterol alone is completely useless. When evaluating a normal cholesterol level for a woman over 60, mainstream guidelines from organizations like the American Heart Association emphasize a nuanced breakdown. Total cholesterol should ideally sit below 200 mg/dL, but if your protective lipids are exceptionally high, a total score of 220 or 240 mg/dL might actually be perfectly safe for your specific physiological makeup. Where it gets tricky is balancing these independent variables against your broader metabolic health.
The Real Story Behind Your LDL and the Particle Size Obsession
We have been taught to view LDL as the ultimate villain in our bloodstream. Except that all LDL particles are not created equal, a nuance that standard cheap lab tests completely obscure. You could have an LDL cholesterol level of 110 mg/dL—technically classified as borderline high—consisting entirely of large, fluffy, buoyant particles that bounce harmlessly off your arterial walls like beach balls. Conversely, another woman might register a seemingly perfect LDL of 85 mg/dL but carry a high concentration of small, dense, pattern B particles that easily penetrate the endothelium and initiate plaque formation. If your physician is only looking at the total mass of LDL rather than ordering an advanced NMR lipoprofile to count the actual particle number, you are making critical health decisions based on incomplete data.
HDL and Triglycerides: The True Power Couple of Female Longevity
For women over sixty, the relationship between high-density lipoproteins and triglycerides is often a far more accurate predictor of cardiac events than LDL could ever hope to be. An ideal HDL level for women is above 50 mg/dL, preferably hovering closer to 60 or 70 mg/dL, as this molecule acts as the cleanup crew, hauling excess fats back to the liver via reverse cholesterol transport. But watch out for your triglycerides, which should ideally remain under 150 mg/dL, or even better, below 100 mg/dL. A skyrocketing triglyceride level combined with plunging HDL is a massive red flag for insulin resistance and metabolic syndrome, a cluster of symptoms that increases female heart attack risk far more aggressively than isolated elevated LDL ever will.
The Often Ignored Danger of High Lipoprotein(a) in Older Adults
There is a silent genetic variant floating around in about 20% of the population that regular lipid panels completely ignore: Lipoprotein(a). This specific particle resembles LDL but possesses an added, highly adhesive protein wrapper that makes it exceptionally prone to causing blood clots and accelerating narrowing of the aortic valve. If you have a stubborn family history of early heart attacks in female relatives, but your standard numbers look pristine, this is likely the culprit. Honestly, it is unclear why this test is not mandatory during every initial post-menopausal screening, considering that diet and traditional statin therapies barely touch Lp(a) levels, requiring entirely different clinical management strategies.
The Great Statins Debate: Are We Over-Medicating Healthy Older Women?
Here is a sharp opinion that makes many conventional cardiologists incredibly uncomfortable: we are aggressively over-prescribing lipid-lowering medications to women over sixty who derive absolutely zero statistical benefit from them. The massive clinical trials that established the benefits of statins—think of landmark studies like the 4S trial or WOSCOPS—were overwhelmingly performed on middle-aged men who already had established coronary heart disease. When researchers look specifically at primary prevention for older women with no history of stroke or heart attack, the data supporting a dramatic reduction in mortality is shockingly thin. Yet, millions of healthy sixty-five-year-old women are started on daily pharmaceuticals the second their total cholesterol ticks past an arbitrary line on a page.
The Flawed Risk Calculators and the ASCVD Miscalculation
When you sit down in your doctor's office, they will likely plug your age, blood pressure, and smoking status into an online tool called the ASCVD Risk Estimator. Because these algorithms heavily weigh chronological age, simply turning 62 automatically bumps your calculated ten-year risk score significantly closer to the treatment threshold. The issue remains that these calculators fail to take into account your physical fitness, dietary quality, or vascular age, treating a vibrant sixty-five-year-old marathon runner with an elevated LDL identical to a sedentary smoker with the same lab values. As a result: thousands of women are coerced into taking medications they do not need based on a rigid mathematical model that ignores individual vitality.
Managing Side Effects: Muscle Pain, Brain Fog, and the Blood Sugar Trap
While statins can be lifesaving for a woman who has already survived a myocardial infarction, the adverse effects for primary prevention can heavily degrade your quality of life. Older women are statistically far more susceptible to statin-induced myopathy—that persistent, deep muscle aching and weakness that makes climbing stairs or lifting groceries a chore. People don't think about this enough, but these drugs can also disrupt glucose metabolism, noticeably increasing your risk of developing type 2 diabetes post-menopause. When you couple that with the frequent complaints of subjective cognitive decline or "brain fog" caused by lowering cholesterol too aggressively in the central nervous system, you have to ask yourself if chasing a perfect lab value is worth sacrificing your daily physical independence.
Beyond the Standard Blood Test: Modern Diagnostics That Actually Matter
If the standard lipid panel is an unreliable metric for predicting your actual risk of a cardiovascular event, what should you actually be asking your physician for during your next checkup? We need to shift our medical focus from measuring the mere presence of fats floating in the bloodstream to visualizing the actual physical state of your arteries. That changes everything, moving the conversation away from hypothetical risk and into concrete, anatomical reality.
The Coronary Artery Calcium Scan: Your True Vascular Roadmap
Instead of guessing how much plaque might be forming based on a blood draw, you can get a direct answer using a quick, non-invasive imaging test called a Coronary Artery Calcium, or CAC, scan. This low-dose X-ray measures the exact amount of calcified plaque in your heart's arteries, returning a score ranging from zero to over a thousand. If you are a 63-year-old woman with a total cholesterol of 260 mg/dL but your CAC score comes back as a perfect zero, your risk of a heart attack over the next decade is exceptionally low, suggesting you can safely avoid pharmaceutical intervention. In short, a CAC scan gives you and your doctor the objective data needed to make a rational, personalized decision rather than playing a game of statistical probabilities.