Understanding PSA: What the Number Actually Represents
PSA stands for prostate-specific antigen—a protein produced by cells in the prostate gland. Its biological job? To liquefy semen so sperm can swim. The thing is, some of that protein leaks into the bloodstream. We measure it with a simple blood test. When levels rise, doctors get curious. Could be inflammation. Could be an enlarged prostate. Could be cancer. Or could be absolutely nothing. The test doesn’t diagnose cancer; it raises flags. And sometimes, it raises false alarms.
How PSA Testing Works in Clinical Practice
Your doctor draws blood, sends it to a lab, and gets a result in nanograms per milliliter (ng/mL). That’s it. No drama. No immediate answers. The real work begins after. A single value is like a still frame from a movie—you need context to understand the scene. A 60-year-old with a PSA of 3.8 ng/mL might be fine. Another man, same age, same number—but with a family history and a rock-hard nodule on exam? That changes everything. The test is cheap, quick, non-invasive. Yet interpreting it demands nuance, experience, and occasionally, restraint.
Why PSA Isn't a Pass/Fail Test
Let’s be clear about this: there’s no universal “normal” PSA. The 4.0 ng/mL cutoff was established in the 1990s based on population averages. But averages lie. Some men have prostate cancer at 2.1. Others live to 90 with no issues at 5.5. The threshold was never a biological boundary—it was a statistical convenience. And because medicine likes clean rules, we ran with it. Now we’re untangling the mess: overdiagnosis, unnecessary biopsies, anxiety for men who mistake a mildly elevated PSA for a death sentence. The data is still lacking on what PSA should be for any individual—and that’s the real problem.
The Age Factor: How Prostate Changes Over Time
By age 60, most men have some degree of prostate enlargement. It’s not cancer. It’s not even dangerous. It’s just biology. The prostate grows throughout life—kind of like how ears keep lengthening, but with more medical consequences. A gland that weighed 20 grams in your 30s might hit 40 or 50 grams by 60. More tissue means more PSA production. So a level of 3.5 or even 4.5 might be perfectly ordinary for a man with a large gland. But you won’t know unless you measure it—via ultrasound or MRI—or track trends over time.
Age-Adjusted PSA Ranges: A More Accurate Picture
Studies from the Prostate Cancer Prevention Trial suggest that average PSA levels creep up with age. At 60, the median is around 1.0 to 1.5 ng/mL—but the upper limit of normal could reasonably be closer to 4.5. Some experts use age-specific ranges: under 2.5 for men 50–59, under 3.5 for 60–69, and under 4.5 for 70+. This makes sense. Yet few primary care doctors apply these refinements. They see “>4.0” and panic. Or worse, they ignore a rising trend because “it’s still under 4.” We’re far from having a one-size-fits-all rule—and we should stop pretending otherwise.
Benign Prostatic Hyperplasia and Its Impact on PSA
Benign prostatic hyperplasia (BPH) affects about 50% of men by age 60. It causes urinary symptoms—frequent trips to the bathroom, weak stream, urgency. And it inflates PSA. A man with moderate BPH might see his PSA jump from 2.0 to 3.8 without any cancer involvement. Treating BPH with medications like finasteride or dutasteride can slash PSA by 50% in six months. So if you’re on one of those drugs, your PSA of 1.5 might actually reflect a “true” level of 3.0. That’s not a typo. That’s biochemistry playing tricks on interpretation. And that’s exactly where doctors need to dig deeper before ordering a biopsy.
When PSA Rises: Not All Spikes Mean Cancer
A sudden PSA increase doesn’t automatically mean tumor growth. Think of the prostate as a sensitive organ—it reacts to irritation. A urinary tract infection? PSA spikes. A bike ride across rough terrain? PSA jumps. A digital rectal exam the day before the blood test? Could bump it up. Even ejaculation within 48 hours can elevate levels slightly. The issue remains: many men get tested without knowing these variables. One-off measurements are practically useless. What matters is velocity—the rate of change over time. A PSA creeping up 0.3 ng/mL per year? Probably benign. One surging from 2.1 to 5.0 in 18 months? That’s a different story.
PSA Velocity and Doubling Time: The Hidden Clues
PSA velocity refers to how fast the number climbs each year. A rise of more than 0.75 ng/mL annually in men over 60 raises red flags. So does a short doubling time—say, less than three years. These metrics often matter more than the absolute value. A man with a PSA of 3.2 but a doubling time of 12 months should worry more than one with 4.5 and stable levels for five years. Yet few clinics calculate these automatically. It requires at least three tests over two years. And because insurance doesn’t always cover frequent testing, we miss these patterns. Which explains why some aggressive cancers slip through while we chase stable elevations.
Inflammation and Infection: Silent PSA Boosters
Prostatitis—prostate inflammation—affects up to 10% of men at some point. It can be bacterial or non-bacterial. Either way, it makes PSA soar. I’ve seen patients with levels hitting 12.0 after a flare-up, only to drop to 2.8 after antibiotics and anti-inflammatories. Biopsying them during the spike would’ve led to a false cancer diagnosis. And that’s not theoretical—it happens. The problem is, symptoms aren’t always obvious. Some men have silent inflammation. No pain. No fever. Just a high PSA. That’s why repeat testing after six to eight weeks is often smarter than jumping to a biopsy.
PSA in Context: Comparing Risk Factors and Alternatives
Imagine two 60-year-old men. Both have a PSA of 4.2 ng/mL. One is African American, has a father who died of prostate cancer, and lives in Detroit. The other is Japanese American, no family history, lives in Hawaii, eats a plant-heavy diet. Are their risks the same? Of course not. Race, genetics, geography, lifestyle—all shape the meaning of a PSA value. Yet most guidelines treat them identically. That’s outdated. Risk-adapted screening is the future. And we’re behind schedule.
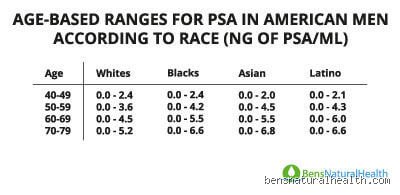
Race and Genetics: Why One Number Doesn’t Fit All
Black men have higher baseline PSA levels and a greater risk of aggressive prostate cancer. Studies show they’re 70% more likely to be diagnosed and twice as likely to die from it. A PSA of 4.0 in a Black man at 60 may warrant earlier investigation than in a white man. Genetic factors like BRCA mutations also tilt the odds. Men with BRCA2 have a higher lifetime risk—up to 27% by age 80—and tend to develop more aggressive forms. Yet genetic testing isn’t routine. Should it be? I find this overrated in low-risk men but underused in those with family histories. Precision beats blanket rules.
Imaging and Biomarker Alternatives to Biopsy
MRI scans have changed the game. A multiparametric MRI can show suspicious areas before a biopsy is ever done. If the scan is clean, a high PSA might be monitored, not attacked. If it shows a lesion, targeted biopsies are more accurate than the old blind 12-core approach. Then there are biomarker tests—like the 4Kscore or PHI (Prostate Health Index)—that combine PSA with other proteins to estimate cancer probability. The 4Kscore, for example, can predict the chance of high-grade cancer with 90% sensitivity. These tests cost $400–$800 and aren’t always covered. But they prevent unnecessary procedures. Suffice to say, we’re no longer limited to “high PSA = biopsy.”
Frequently Asked Questions
Should All 60-Year-Old Men Get a PSA Test?
No. The U.S. Preventive Services Task Force recommends shared decision-making. That means discussing risks and benefits with your doctor. PSA screening reduces prostate cancer mortality by about 20–30% over 10 years—but at the cost of overdiagnosis. For every 1,000 men screened, roughly 240 will have an elevated PSA. Of those, 100 will get biopsied. And only 30–40 will actually have cancer. Of those, 10–15 will have aggressive disease. The rest? Indolent tumors that might never have caused harm. So the question isn’t “should you test?”—it’s “are you prepared for the consequences of the result?”
Can Medications Affect PSA Levels?
Absolutely. Finasteride (Proscar) and dutasteride (Avodart), used for BPH, reduce PSA by about 50% within six months. If you’re on one, your doctor should double your PSA when interpreting it. Tamsulosin (Flomax)? Doesn’t affect PSA. Antibiotics for prostatitis? Can lower it significantly. Even herbal supplements like saw palmetto may have a modest effect. The issue remains: patients often don’t tell doctors about supplements. Miscommunication skews interpretation. Always disclose everything.
What Happens After a High PSA Reading?
First step? Don’t panic. Repeat the test. Rule out infection. Avoid ejaculation and cycling for 48 hours before. If it’s still high, consider an MRI. If the MRI shows something suspicious, a targeted biopsy follows. If not, watchful waiting with repeat tests every 6–12 months may be wiser. A biopsy isn’t harmless—it carries risks of infection (1–2%), bleeding, and anxiety. Because of this, rushing into one is rarely the best move. And that’s exactly where patient education makes the difference.
The Bottom Line
A normal PSA for a 60-year-old isn’t a single number—it’s a range, a trend, a story shaped by genes, habits, and prostate biology. The old 4.0 ng/mL rule is outdated, overly simplistic, and often misleading. We need to stop treating PSA like a verdict and start seeing it as a conversation starter. Tracking changes over time, combining it with imaging and risk factors, and avoiding knee-jerk biopsies—that’s smarter medicine. I am convinced that personalized screening, not universal thresholds, is the path forward. Will every man need a PSA test at 60? No. But every man should understand what the test can—and can’t—tell him. Because when it comes to prostate health, ignorance isn’t peace. It’s risk disguised as comfort.