When someone receives a Parkinson's diagnosis in a clinic—whether at the Mayo Clinic or a local neurology practice—the immediate panic usually centers on the physical manifestations. The resting tremor. The shuffling gait. The rigid posture that makes tying a shoe feel like climbing Everest. Yet, under the surface, a silent clock is ticking for many, though certainly not all, patients.
The Messy Reality of a Parkinson’s Diagnosis: More Than Just Shaking
Parkinson’s disease is traditionally defined by the death of dopamine-producing neurons in a specific region of the brain called the substantia nigra. But that definition is criminally incomplete. I argue that we have done patients a massive disservice by labeling this exclusively as a movement disorder because it sets up a false sense of security regarding mental sharpness.
The Alpha-Synuclein Invasion
What is actually happening? It comes down to a rogue protein called alpha-synuclein. In a healthy brain, this protein is harmless, but in Parkinson’s, it misfolds and clumps into toxic aggregates known as Lewy bodies. These cellular wrecking balls do not just stay cooped up in the brainstem. They march. They spread outward into the cerebral cortex—the very seat of human memory, planning, and abstract thought—which explains why the physical disease can eventually morph into a cognitive one. That changes everything.
The Disappearing Act of Acetylcholine
Everyone talks about dopamine, yet the real culprit behind the cognitive slide is often a completely different neurotransmitter called acetylcholine. While dopamine loss ruins your ability to walk smoothly, acetylcholine depletion destroys your ability to pay attention or recognize your surroundings. The issue remains that standard treatments like levodopa do absolutely nothing to fix this second chemical drought. Because of this, a patient might have perfectly controlled physical tremors thanks to their medication, while their ability to manage a checkbook simultaneously goes out the window.
Tracking the Timeline: When Parkinson's Disease Dementia Takes Hold
Timing is everything in neurology. If cognitive decline shows up decades after the first hand tremor, it is classified as Parkinson’s disease dementia, a trajectory that follows a very specific, agonizingly slow burn.
The One-Year Rule That Splintered Neurology
Doctors rely heavily on an arbitrary chronological boundary known as the "one-year rule" to differentiate between related conditions. If the motor symptoms have been established for at least 12 months before any major cognitive impairment rears its head, the official diagnosis is PDD. Is this timeline perfect? Honestly, it's unclear, and many movement disorder specialists openly disagree on whether this distinction even matters in a practical clinical setting since the underlying cellular damage looks almost identical under a microscope.
Predictors of the Shift: Who is Most at Risk?
Not every patient faces the same odds. Age is the most aggressive risk factor here; an individual diagnosed at age 50 faces a radically different cognitive prognosis than someone diagnosed at 78. A famous 2003 longitudinal study conducted in Sydney, Australia, tracked patients over 20 years and revealed that older age at onset, coupled with early hallucinations and severe baseline rigidity, predicted a much faster slide toward PDD. People don't think about this enough, but if a patient experiences vivid visual hallucinations within the first few years of their physical diagnosis, it usually means the Lewy bodies have already breached the cortex.
The Biological Blueprint: How Brain Changes Trigger PDD
To understand why this transition happens, we have to look at the brain as an electrical grid where several major power stations are failing at the same time.
The Frontal-Subcortical Disconnect
The human brain relies on complex loops that connect the deep, primitive movement centers to the advanced prefrontal cortex. In PDD, these loops are severed. This results in an executive dysfunction that looks very different from typical memory loss. A patient might remember what they did in 1965 with crystal clarity, but give them a simple three-step instruction—like "pick up the keys, unlock the blue door, and sit down"—and their brain stalls out entirely. Where it gets tricky is that the information is still inside their head; the brain simply lacks the processing power to retrieve it on command.
The Role of Chronic Neuroinflammation
We cannot ignore the immune system's role in this neurological breakdown. When Lewy bodies accumulate, they trigger an aggressive response from microglia, the brain’s resident immune cells. Instead of clearing the toxic proteins, these cells go into overdrive, secreting inflammatory cytokines that accidentally poison nearby healthy neurons, which explains why the cognitive decline can sometimes accelerate rapidly after a physical trauma or a severe urinary tract infection. The thing is, the brain is essentially fighting a war against itself, and the collateral damage is the patient's intellect.
The Ultimate Diagnostic Clash: Parkinson’s Dementia vs. Alzheimer’s Disease
It is incredibly common for families to mistake PDD for Alzheimer's disease, but treating them as the same entity is a dangerous medical mistake.
Contrasting the Cognitive Profiles
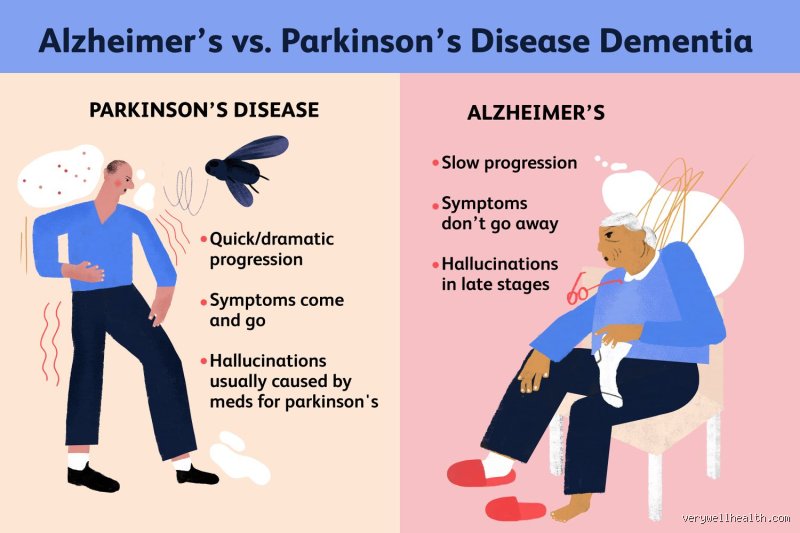
Alzheimer’s is fundamentally a disease of storage; the brain’s filing cabinets are physically destroyed by amyloid plaques and tau tangles, meaning new memories cannot be formed. Parkinson’s dementia, conversely, is a failure of retrieval. It is like having a perfectly functional filing cabinet but the clerk working the desk has gone on an infinite lunch break. Furthermore, while an Alzheimer's patient might struggle to find the right words, a PDD patient is much more likely to experience profound spatial disorientation, such as getting lost inside a house they have lived in for 40 years.
Fluctuations and the Daylight Phenomenon
Perhaps the most bizarre and heartbreaking characteristic of PDD is the unpredictable, fluctuating nature of the cognitive impairment. A patient might be totally incoherent at 9:00 AM, unable to recognize their own spouse, only to become completely lucid, sharp, and conversational by lunchtime. You won't see that specific roller-coaster profile in typical Alzheimer's. This erratic shifting creates an emotional minefield for caregivers, who often wonder if their loved one is simply "faking it" or not trying hard enough, though we are far from it being a matter of willpower.
Common mistakes and misconceptions about Parkinson's disease dementia
Confusing Lewy body dementia with Parkinson's dementia
People throw these terms around like they are interchangeable twins. They are not. The difference hinges entirely on a cruel stopwatch. If cognitive decline cripples a patient a year or more after motor issues like tremors lock up the limbs, we call it Parkinson's disease dementia. But what if memory failure strikes first, or simultaneously? Then you are dealing with Dementia with Lewy Bodies (DLB). Both conditions feature abnormal alpha-synuclein protein deposits, yet the chronological trajectory dictates the diagnosis. Why does this matter? Because misjudging the timeline misdirects the therapeutic strategy, leaving families blindsided by completely unexpected behavioral storms.
Assuming memory loss is the primary initial symptom
Alzheimer's has conditioned us to look for forgotten keys and erased names. Parkinson's dementia plays a completely different, more insidious game. The problem is that early cognitive erosion here targets executive function and visuospatial awareness rather than short-term recall. A patient might remember what they ate for breakfast in vivid detail. However, they suddenly cannot organize a simple checkbook, judge the distance to the kitchen table, or navigate a familiar hallway. It is a failure of processing speed and mental flexibility, not a blank hard drive. Families often miss these red flags because the individual still tracks conversations perfectly well.
Believing dementia is an inevitable destination
Let's be clear: a Parkinson's diagnosis is not an automatic ticket to severe cognitive oblivion. Statistics show that roughly 30% of individuals with Parkinson's do not develop significant dementia even after living with the movement disorder for decades. Risk factors like advanced age, severe rigidity, and early hallucinations heavily influence the outcome. Does Parkinson's turn into dementia for every single person? No, it does not. Assuming total cognitive collapse is a guarantee creates unnecessary, paralyzing terror for newly diagnosed patients who could otherwise enjoy many highly functional, lucid years.
The overlooked impact of nighttime disruptions on cognition
The REM sleep behavior disorder link
Neurologists often fixate on daytime tremors while ignoring what happens when the sun goes down. A strange phenomenon known as REM Sleep Behavior Disorder (RBD) causes patients to physically enact violent dreams. They kick, thrash, and scream because the brain's natural sleep paralysis mechanism breaks down. Recent longitudinal data reveals that over 80% of Parkinson's patients with RBD eventually face cognitive decline. This nocturnal chaos is not just a nuisance; it is a profound diagnostic warning sign. The issue remains that chronic sleep fragmentation starves the cerebral cortex of deep restorative cycles, which explains why daytime cognitive processing plummets after a rough night.
Proactive tracking of sleep architecture
Instead of waiting for memory scores to drop during annual clinic visits, families should aggressively monitor nighttime behaviors. Early identification of sleep disturbances allows for targeted interventions using melatonin or clonazepam. Which brings us to an uncomfortable truth: suppressing these vivid nightmares does not cure the underlying pathology, but it preserves precious daytime alertness. We must look at the bedroom as a neurological laboratory. If we manage the nighttime turbulence early, we protect the patient's immediate quality of life and potentially buffer the brain against rapid, exhausting executive decline.
Frequently Asked Questions
Does Parkinson's turn into dementia in the early stages of the disease?
Cognitive decline rarely dominates the initial phase of a Parkinson's diagnosis. Clinical registries indicate that fewer than 10% of patients exhibit significant dementia within the first three years of motor symptom onset. Instead, early mild cognitive impairment might cause subtle sluggishness in decision-making or mild multi-tasking difficulties. The risk accelerates dramatically later, with the average onset of dementia occurring roughly 10 to 15 years after the initial physical tremors manifest. Therefore, early stage slip-ups are usually attributable to medication side effects or sleep deprivation rather than permanent cortical destruction.
Can lifestyle modifications delay the progression of cognitive decline in Parkinson's?
Rigorous physical exercise stands out as the most potent non-pharmacological weapon we currently possess. Studies tracking Parkinson's populations show that 150 minutes of moderate-to-vigorous aerobic activity weekly correlates with a 35% reduction in cognitive worsening over time. Physical movement triggers the release of brain-derived neurotrophic factor, essentially acting as fertilizer for vulnerable neurons. Combined with a Mediterranean diet rich in antioxidants and aggressive management of vascular health, exercise actively fortifies the brain's remaining neural networks. But can a treadmill completely stop genetic predisposition? Exceptional efforts help immensely, yet they cannot entirely veto aggressive alpha-synuclein pathology if the disease is fiercely progressive.
How do doctors differentiate between Parkinson's dementia and Alzheimer's disease?
Physicians rely on distinct clinical profiles and neuropsychological testing batteries to separate these two neurodegenerative giants. Alzheimer's patients typically present with profound amnesia, struggling to retain new information even when given helpful contextual cues. Conversely, an individual tracking toward a Parkinson's disease dementia diagnosis can usually retrieve memories when prompted, proving the data is stored but simply hard to access. Furthermore, visual hallucinations, dramatic fluctuations in daily alertness, and severe motor dysfunction are hallmark traits of Parkinson's-related cognitive failure. Alzheimer's patients generally maintain normal physical gait and motor control until the final, advanced stages of their disease journey.
A definitive perspective on the Parkinson's cognitive trajectory
We must stop treating the cognitive aspects of Parkinson's disease as a taboo footnote to a movement disorder. The reality is stark: mental erosion represents the single greatest burden on caregivers and the primary driver of nursing home placements. Medical communities often sugarcoat this progression to maintain patient optimism, but false hope serves no one when legal and financial planning hang in the balance. Does Parkinson's turn into dementia? For a significant majority of long-term survivors, the answer is yes, and we must confront that reality with aggressive, early intervention rather than passive resignation. Our clinical focus needs a massive paradigm shift away from merely suppressing hand tremors and toward fiercely defending executive brain function. Only by acknowledging the true scale of this cognitive threat can we allocate the research funding and specialized care infrastructure required to handle the oncoming neurological tide.