The Hidden Reality of Parkinson's Disease Dementia and Cognitive Decline
We all visualize the same thing when the condition comes up. The shaky hand, the frozen gait, the slow, deliberate steps across a room—the classic motor symptoms described by James Parkinson back in 1817. But that is just the surface. The thing is, this condition is as much a disease of the mind as it is of the muscles, yet the cognitive aspects get brushed under the rug because the physical tremors are so visually dominant. For decades, the medical community treated the cognitive side as an afterthought, an unfortunate footnote that only mattered in the final stages of the illness.
Moving Beyond the Motor Symptoms to the Basal Ganglia
The core problem originates deep within the basal ganglia, specifically inside a dark sliver of tissue called the substantia nigra. This is where your brain manufactures dopamine, a neurotransmitter that acts like oil in a complex mechanical engine. When these dopamine-producing neurons die off—often dropping by 60% to 80% before a single physical symptom even shows up—the entire neurological highway system grinds to a halt. But dopamine does not just control your ability to walk smoothly. It also fuels the prefrontal cortex, which is essentially the master control center for your working memory, attention span, and ability to switch between complex tasks without losing your train of thought.
Why the Term Dementia Misleads the Public
When doctors throw around the word dementia, people immediately panic and picture late-stage Alzheimer’s disease. Except that Parkinson’s disease dementia involves an entirely different set of behavioral rules. It is not about forgetting your daughter's name or getting lost in the house you lived in for forty years. Instead, it manifests as a profound slowing of mental processing, a frustrating condition known as bradyphrenia. Patients know exactly what they want to say, but the neural bridge connecting the thought to the vocal cords feels like it has been coated in thick molasses. Honestly, it's unclear why some patients experience rapid mental decline while others remain sharp as a tack for decades, and experts disagree fiercely on the exact tipping points.
The Dopamine Drought: How Chemical Depletion Alters Working Memory
Think of your working memory as a sticky note on a crowded desk. It holds temporary information—like a phone number you just read or the reason you walked into the kitchen—just long enough for you to do something with it. In a healthy brain, dopamine keeps that sticky note firmly attached to the desk. But during a dopamine drought, the note blows away before you can read it. It is a terrifying realization when you suddenly find yourself standing in the middle of a room with absolutely no clue what you were searching for. That changes everything about how a person navigates their daily routine.
The Frontal-Striatal Network Breakdown
The communication line between the striatum and the prefrontal cortex is called the frontal-striatal network. When dopamine vanishes, this specific pathway starts misfiring completely, which explains why multitasking becomes an absolute nightmare for these individuals. Imagine trying to juggle three spinning plates, but someone suddenly turns off the lights in the room. But what happens when the brain tries to compensate? It reroutes signals through less efficient neural pathways, burning massive amounts of metabolic energy just to accomplish basic cognitive tasks that used to require zero conscious effort. As a result: patients experience intense mental fatigue by mid-afternoon, rendering them completely incapable of making complex financial or medical decisions.
Executive Dysfunction Versus Simple Forgetfulness
Where it gets tricky is separating everyday absentmindedness from true executive dysfunction. If you lose your car keys because you were distracted while walking through the front door, that is just normal human error. But if you are staring directly at your car keys on the kitchen counter and your brain simply cannot formulate the step-by-step sequence required to pick them up, unlock the vehicle, and navigate to the grocery store, you are dealing with a severe breakdown of executive control. It is an issue of organization and initiation. The memory itself is not actually gone from the brain's storage banks; rather, the biological retrieval mechanism has been utterly compromised by the disease.
The Disastrous Impact on Spatial Awareness
People don't think about this enough, but memory is deeply tied to how we perceive space and geometry. Parkinson’s ravages visual-spatial processing, meaning the brain struggles to accurately calculate distances or visualize three-dimensional objects in the mind's eye. A study conducted at the University College London in 2022 revealed that patients with advanced Parkinson’s frequently misjudge the height of curbs or the depth of doorways, leading to dangerous trips and falls. This is not a visual problem with the eyes themselves—it is a processing failure within the parietal lobe, which relies heavily on dopaminergic inputs to map the physical world accurately.
Lewy Bodies and the Aggressive Trajectory of Cognitive Change
Dopamine depletion is only half the story. The real villain behind severe, irreversible memory loss in this population is the widespread accumulation of abnormal protein deposits called Lewy bodies. These toxic clumps are composed primarily of a misfolded protein called alpha-synuclein, which behaves like a microscopic weed, choking out healthy brain cells and disrupting electrical communication across entire cortical networks. When these proteins remain confined to the brainstem, you mostly see physical tremors and rigidity; however, once they migrate upward into the cerebral cortex, the cognitive architecture of the brain begins to crumble rapidly.
The Diagnostic Timing Dilemma
This brings us to a critical fork in the diagnostic road. If a patient develops prominent motor symptoms first, and then exhibits signs of memory failure at least one year later, they receive a diagnosis of Parkinson’s disease dementia. But if the memory loss, vivid visual hallucinations, and severe confusion show up before or alongside the physical tremors, the diagnosis flips to Dementia with Lewy Bodies (DLB). It might seem like semantic hair-splitting to an outsider, but the clinical trajectory and treatment responses for these two conditions are wildly different. We're far from it being a unified, easy-to-treat diagnosis.
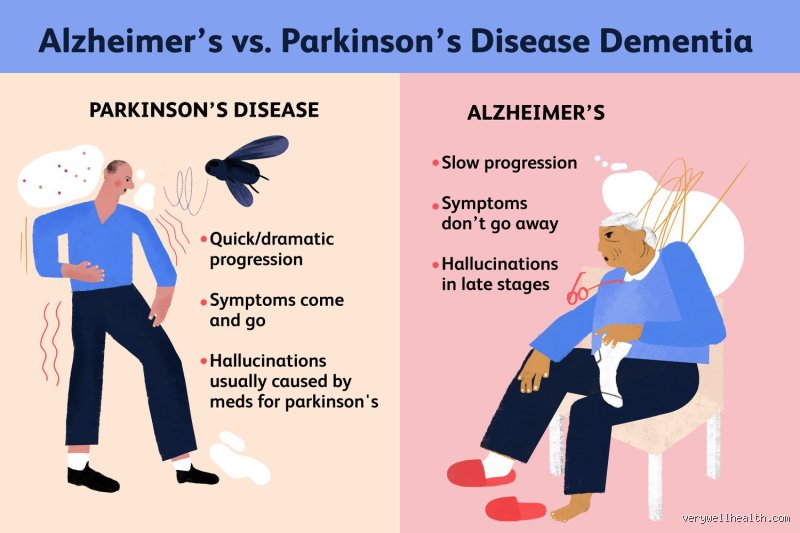
Distinguishing the Cognitive Profiles: Parkinson's vs. Alzheimer's
To truly understand how Parkinson’s affects memory, you must look at how it contrasts with the heavyweight champion of cognitive decline: Alzheimer’s disease. I am always struck by how differently these two conditions behave in a clinical setting. Alzheimer's is a destructive bulldozer that target the hippocampus—the brain's primary recording studio—meaning new memories are never even saved in the first place. Parkinson’s, conversely, damages the retrieval machinery, leaving the underlying memories largely intact but locked away behind a door that won't open. The following matrix illustrates these stark neurological differences across key diagnostic categories.
The Power of Biological Hinting
This structural difference is why a simple cueing experiment can tell a neurologist so much during an examination. If you ask an Alzheimer’s patient what they ate for breakfast yesterday, they cannot tell you, and even if you give them a list of multiple-choice options, they will guess randomly because the event was never recorded by the damaged hippocampus. But if you ask a Parkinson’s patient the exact same question, they might stare blankly for a long moment, scratching their chin while struggling to find the words—yet the moment you say, "Was it oatmeal or eggs?", their eyes light up and they instantly pick the correct answer. The clue provides the external steering mechanism that their own frontal lobe can no longer generate independently, proving conclusively that the memory was safely stored away all along.
Common mistakes and misconceptions about Parkinson's memory decline
The Alzheimer's conflation trap
People hear the word forgetfulness and immediately jump to Alzheimer's disease. Except that the neurological machinery failing here is entirely different. While Alzheimer’s ravages the hippocampus to erase the data itself, Parkinson's impairs the prefrontal cortex, which acts like a rusty search engine. The memory sits in the brain, but the retrieval mechanism stalls. Does Parkinson's affect memory in the exact same catastrophic, identity-erasing way early on? No. We are dealing with an efficiency deficit, not a complete structural deletion of your past layout.
Assuming motor symptoms always precede cognitive shifts
Waiting for a severe tremor before checking mental acuity is a massive miscalculation. Subcortical dementia manifestations can sneak into the picture long before the physical shuffle becomes obvious. Bradyphrenia, which explains the agonizingly slow processing speed patients endure, often gets misdiagnosed as simple aging or depression. The issue remains that clinical focus fixates heavily on dopamine pathways regulating movement. Meanwhile, acetylcholine networks quietly wither in the background, fracturing a patient's working memory.
The myth of universal, inevitable amnesia
Let's be clear: a diagnosis is not a guaranteed ticket to profound cognitive oblivion. Statistics show about 40 percent of individuals with Parkinson's navigate their daily routines without experiencing debilitating memory impairments. Assuming every patient will lose their cognitive footing breeds unnecessary panic. It alters how families interact with patients, sometimes suffocating their independence prematurely. Why throw away autonomy based on a statistical flip of a coin?
The sleep-cognition axis: An overlooked expert lever
Targeting REM sleep behavior disorder
The real battle for cognitive preservation happens when the eyes are closed. An astonishing 50 to 60 percent of Parkinson's patients suffer from REM Sleep Behavior Disorder (RBD), a condition where they physically enact vivid dreams due to a lack of muscle atonia. This is not just an annoying nighttime disruption. This violent sleep fragmentation actively accelerates neurodegeneration. When you fail to achieve deep, restorative sleep phases, the brain cannot clear metabolic waste like alpha-synuclein aggregates. As a result: the cognitive reserve plummets exponentially faster than it would under normal conditions.
Neurologists now view aggressive sleep optimization as a frontline defense strategy. Managing RBD through targeted therapies or specialized melatonin protocols does more than just quiet the nights; it actively buffers the neural networks handling executive functions. If we ignore sleep quality, even the most sophisticated dopaminergic drug regimens will fail to protect working memory pathways. It is an unyielding biological tax that must be paid.
Frequently Asked Questions
Does Parkinson's affect memory differently than normal aging?
Natural senescent decline typically manifests as mild, occasional forgetfulness, like misplacing a set of car keys for an hour. Conversely, Parkinson's cognitive impairment targets executive operations, making it incredibly difficult to sequence complex tasks like managing a multi-tiered financial budget or navigating familiar driving routes. Data indicates that while normal aging slows recall by a small fraction, up to 80 percent of those with Parkinson's will develop recognizable cognitive deficits over a 20-year disease trajectory. The problem is a systemic breakdown in attention switching rather than a benign, age-related processing delay. This specific cognitive decay requires distinct diagnostic toolsets to differentiate it from standard geriatric slowdowns.
Can lifestyle modifications actively preserve memory recall in patients?
Rigorous clinical trials demonstrate that high-intensity aerobic exercise increases brain-derived neurotrophic factor (BDNF), a vital protein supporting neuronal survival. Engaging in 150 minutes of moderate exercise weekly has been shown to measurably stabilize cognitive trajectories over a two-year period compared to sedentary control groups. But physical movement alone is insufficient, which explains why specialists advocate for simultaneous cognitive training and adherence to a strict Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet. Cognitive engagement must be novel and frustratingly complex (like learning a brand-new dialect or a complex instrument) to actually force the brain to sprout alternative neural pathways. Relying solely on repetitive crosswords will not cut it when fighting systemic neurological decline.
When should a family seek a formal neuropsychological evaluation?
You should schedule comprehensive baseline testing the moment subtle behavioral shifts begin disrupting routine occupational or social functioning. Waiting until a patient forgets the names of immediate family members or gets hopelessly lost in their own neighborhood is a critical mistake. Early tracking utilizing tools like the Montreal Cognitive Assessment provides a concrete numerical baseline to measure future decline against. Because anxiety and clinical depression mimic cognitive failure by artificially suppresses attention spans, a formal evaluation untangles emotional distress from actual structural neurodegeneration. Identifying these nuances early allows for timely pharmacological interventions before the damage becomes completely irreversible.
A definitive stance on the Parkinson's cognitive crisis
We must stop treating cognitive decline as a secondary footnote to the physical tremors of this disease. The medical community routinely obsesses over gait and rigidity while allowing the stealthy erosion of a patient's intellect to go unaddressed for years. This systemic negligence strips individuals of their agency long before their bodies completely give out. Does Parkinson's affect memory? Absolutely, and it does so with a insidious subtlety that demands aggressive, early cognitive intervention rather than passive observation. True patient care requires us to fiercely defend the mind with the exact same therapeutic urgency we use to stabilize the body.