The Illusion of the Steady Decline: What Really Happens Beneath the Surface
Neurologists love to talk about the Hoehn and Yahr scale, a classic clinical rating system developed in 1967 that maps the progression of Parkinson’s across five neat, sequential stages. It looks beautiful on a PowerPoint slide at a medical conference. In the clinic, however, patients do not live in neat stages; they experience a disease that feels like a staircase with wildly uneven steps. Subclinical neurodegeneration progresses quietly for years while the brain utilizes its immense compensatory mechanisms to mask the damage. You lose up to 60% of your dopamine-producing neurons in the substantia nigra before the very first hand tremor even registers. Think of it like a dam holding back a massive reservoir; the concrete cracks slowly, invisibly, until one day a tiny shift causes the whole structure to weep water.
The Myth of the Linear Progression
The thing is, we have been conditioned to expect chronic illness to behave like a smoothly descending ramp. It doesn't. A patient in Chicago might spend four years with nothing more than a mild dragging of the left foot and a muted facial expression, only to wake up one Tuesday unable to rise from bed unaided. Is this a sudden biological acceleration of the disease itself? Honestly, it's unclear in the absolute strictest sense of cellular pathology, but clinically, the impact is identical. Experts disagree on whether the brain simply runs out of backup pathways or if external triggers rewrite the rules of the game overnight, but the outcome for the family is a sudden, terrifying shift in reality.
When the Brain Runs Out of Tricks
Our neural networks are shockingly resilient. When dopamine levels drop, adjacent circuits alter their firing patterns to pick up the slack—a phenomenon known as functional plasticity. But this coping mechanism has a hard ceiling. What happens when the brain hits that threshold? The drop-off is steep. It is less like a fading light bulb and more like a fuse blowing. Once those reserve pathways are exhausted, the clinical presentation shifts dramatically, making a long-standing, slow-burning disease look like a sudden catastrophe.
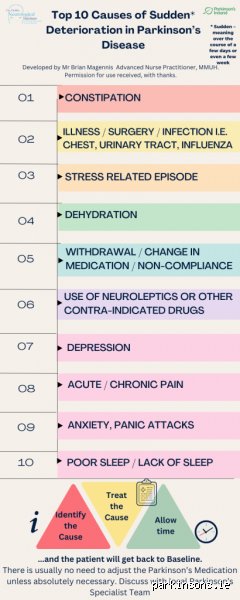
The Hidden Catalysts Behind an Abrupt Parkinsonian Crash
When a person with Parkinson's experiences a sudden worsening of mobility, cognition, or speech over days or hours, looking at the brain is actually the wrong place to start. We must look at the rest of the body. An acute change in status almost always signals a secondary medical event that has hijacked the nervous system. The brain, already starved of dopamine, simply lacks the biochemical resilience to handle any extra systemic friction.
The Urinary Tract Infection Trajectory
Ask any seasoned geriatric nurse at Mount Sinai Hospital in New York what the number one cause of sudden neurological decline in elderly patients is, and they will answer without a second of hesitation: an asymptomatic urinary tract infection. In a healthy thirty-year-old, a UTI causes localized discomfort. In a seventy-year-old with Parkinson’s, that same bacterial colonization triggers a massive, systemic inflammatory response. Pro-inflammatory cytokines cross the blood-brain barrier, temporarily crippling an already compromised basal ganglia. The result is a terrifying cocktail of acute delirium, severe rigidity, and a total loss of postural stability. And yet, once the proper course of antibiotics clears the infection, the patient often returns right back to their baseline within seventy-two hours, proving that the underlying Parkinson’s did not actually worsen, even though it looked exactly like it did.
The Pharmacy Tightrope and Cognitive Traps
Where it gets tricky is the delicate balancing act of dopaminergic medication. A tiny, seemingly trivial shift in dosing schedules can cause a massive clinical collapse. If a caregiver accidentally gives a dose of carbidopa-levodopa forty-five minutes late, or if a change in gastric motility prevents the stomach from absorbing the drug properly, the patient can experience a profound "off" period that mimics a permanent, catastrophic decline. Furthermore, we must talk about the dark side of common medications. If a well-meaning emergency physician prescribes a standard anti-nausea drug like metoclopramide during a bout of stomach flu, they are unwittingly administering a potent dopamine receptor antagonist. That changes everything. Within hours, the patient can become entirely catatonic, immobilized by a drug interaction rather than the disease itself.
The Trauma of Modern Hospitalization
Hospital environments are inherently hostile to the Parkinsonian brain. The flashing lights, the disrupted sleep architecture, the unfamiliar faces, and the inevitable delays in medication delivery create a perfect storm for acute delirium. A 2022 study tracking Parkinson's admissions found that over 35% of patients experienced a severe, sudden worsening of symptoms during a hospital stay for an unrelated issue like a broken bone or pneumonia. The sheer psychological and physiological stress of a new environment acts as a chemical magnifier for every underlying motor deficit.
Decoupling True Progression from Secondary Medical Crises
We need to establish a clear distinction between a permanent neurological shift and a temporary fluctuation, even if they look identical through a caregiver's eyes. True disease progression takes months or years to cement itself into the nervous system. A sudden drop over the weekend is almost always a diagnostic SOS from elsewhere in the body.
The 48-Hour Diagnostic Window
When analyzing a sudden dip in function, time is our most valuable diagnostic tool. Did the inability to swallow develop over the course of six months, or did it manifest right alongside a new cough? If the decline occurs within a forty-eight-hour window, the primary suspect should never be the natural evolution of Parkinson’s. Neurologists rely on this temporal profile to separate the signal from the noise. People don't think about this enough: a rapid descent is actually a reason for hope, because acute causes are usually treatable, whereas the slow, true progression of the disease is a much tougher beast to fight.
The Biomarkers of Acute Stress
To unravel this mystery, clinicians rely on a rapid battery of tests rather than brain imaging. Elevated white blood cell counts, high levels of C-reactive protein, or abnormalities in serum electrolytes provide immediate clues. A brain MRI rarely tells you why a Parkinson’s patient suddenly stopped walking yesterday, but a simple blood draw or metabolic panel usually reveals the culprit immediately. We are far from having a simple finger-prick test for Parkinson's progression, so we must rely on these indirect systemic markers to rule out the external chaos first.
Parkinson’s Versus atypical Parkinsonism: A Vital Distinction in Sudden Decline
But what if there is no infection? What if the medications are perfectly balanced, the lab work is pristine, and yet the patient is still sliding down a steep hill? This is where we have to question the original diagnosis itself. Parkinson's disease is frequently confused with a cluster of conditions known as atypical Parkinsonian syndromes or "Parkinson-plus" disorders, which behave very differently from the classic condition.
The Aggressive Trajectory of Multiple System Atrophy
Multiple System Atrophy, or MSA, is a brutal mimic that initially presents almost identically to standard Parkinson’s disease. However, the issue remains that MSA does not play by the same rules of slow progression. Patients with MSA often experience a rapid, relentless deterioration of the autonomic nervous system within the first two years of symptom onset. They suffer from severe, sudden drops in blood pressure upon standing, early urinary incontinence, and a total lack of response to traditional levodopa therapy. If a patient is declining at a speed that terrifies their medical team, a re-evaluation of the diagnosis is vital.
Progressive Supranuclear Palsy and the Danger of Early Falls
Another classic imposter is Progressive Supranuclear Palsy, which targets eye movements and balance much earlier and more aggressively than standard Parkinson’s. While a typical Parkinson’s patient might struggle with falls a decade into their diagnosis, a person with PSP might start falling backward, unexpectedly, in the very first year. Which explains why a sudden increase in injury frequency often points toward this alternative pathology. It is a completely different neurological landscape, hence the absolute necessity of tracking the precise nature of these sudden physical failures rather than lumping them under a single, generic umbrella.
Common Mistakes and Misconceptions Regarding Sudden Declines
Family caregivers often trap themselves in a devastating assumption. When a loved one with Parkinson's suddenly loses the ability to walk or speak clearly over a weekend, panic dictates that the underlying neurodegenerative disease has leaped into an aggressive, irreversible phase. Let's be clear: idiopathic Parkinson's disease does not operate like that. It moves with a glacial, agonizing slowness. A sudden crash in functionality is almost never a permanent escalation of the structural brain pathology itself, but rather a systemic distress signal masking as disease progression.
The Illusion of a Broken Brain
People assume the dopamine-producing neurons in the substantia nigra just vanished overnight. They did not. When you observe a catastrophic drop in mobility, the true culprit is typically a secondary metabolic insult. An underlying urinary tract infection, severe dehydration, or even acute constipation can completely disrupt the delicate neurochemical equilibrium of a vulnerable brain. Medical professionals frequently witness patients presenting with profound delirium and rigid immobility who miraculously return to their baseline once their systemic infection is cured with targeted antibiotics. Confusing these acute, treatable episodes with true disease progression leads to therapeutic nihilism where families give up hope prematurely.
The Myth of Constant Medication Failure
Another frequent misstep is blaming the sudden worsening of symptoms entirely on drug tolerance. Families look at a patient freezing in place and deduce that the levodopa has permanently stopped working. Except that the gastrointestinal tract in Parkinson's is notoriously erratic. Gastroparesis, which delays stomach emptying, can cause oral medications to sit stranded in the gut for hours. If the carbidopa-levodopa cannot reach the proximal small intestine for absorption, a sudden and terrifying "off" period occurs. It is not that the brain is suddenly immune to the medication; rather, the mechanical delivery system has stalled, a nuance that demands dietary adjustments or prokinetic therapies instead of blind dose escalations.
The Hidden Impact of Silent Stressors and Advanced Management
Beyond the typical infection or digestive bottleneck, a less understood driver of rapid physical decline is psychological trauma or abrupt environmental dislocation. The Parkinsonian brain possesses an incredibly fragile compensatory framework.
The Neurochemical Cost of Relocation Shock
Moving a patient from their familiar home environment into an assisted living facility or a hospital ward frequently triggers a sudden, severe decompensation. This phenomenon, sometimes called relocation stress syndrome, induces a massive cortisol surge that actively interferes with remaining dopaminergic transmission. The patient might go from independent ambulation to being completely wheelchair-bound within forty-eight hours of admission. Why does this happen? The loss of familiar spatial cues forces the brain to rely on conscious, executive cognitive processing to execute basic motor tasks like walking, an exhausting workaround that fails instantly under acute emotional duress. Recognizing this allows specialists to implement strict environmental stabilization protocols rather than altering drug regimens aggressively.
Optimizing the Absorption Window
Expert management requires looking closely at what happens at the dinner table. Dietary protein competes directly with levodopa for the same transport carriers across the intestinal wall and the blood-brain barrier. If a patient suddenly changes their eating habits and consumes a high-protein lunch, their afternoon medication might be entirely neutralized. This can mimic a sudden neurological collapse. To combat this, clinicians advocate for a protein-redistribution diet, where the bulk of daily protein intake is shifted exclusively to the evening meal, thereby keeping the daytime absorption channels entirely unobstructed for optimal motor control.
Frequently Asked Questions
Can Parkinson's deteriorate suddenly due to a change in routine?
Yes, because structural changes in the basal ganglia make adapting to new environments exceptionally difficult. A sudden alteration in daily structure or sleep deprivation can cause an immediate, temporary plunge in both cognitive and motor performance. Clinical observations indicate that up to forty percent of Parkinson's patients experience measurable behavioral or physical regression when their micro-routines are disrupted. The issue remains that the brain has lost its automated processing abilities, meaning any added cognitive load or stress drains the limited neural resources available for movement. Fortunately, restoring the predictable routine almost always reverses this specific type of sudden decline within a few days.
How do doctors differentiate between a true disease progression and an acute medical event?
Physicians rely heavily on the timeline of symptom onset and targeted diagnostic testing to untangle this dilemma. True disease progression unfolds subtly over many months or years, whereas a localized infection, a silent stroke, or a toxic drug interaction manifests within hours or days. Medical teams will immediately order a comprehensive metabolic panel, urinalysis, and blood cultures to check for systemic inflammation or electrolyte imbalances. If a patient presents with sudden confusion alongside worsened tremors, elevated white blood cell counts or abnormal sodium levels point directly toward a treatable medical event rather than an escalation of Parkinson's itself. Which explains why an abrupt change should always prompt a trip to the clinic rather than a resigned acceptance of a new normal.
Is a sudden increase in falls a sign that the disease has entered its final stage?
Not necessarily, though it demands immediate investigation because falls represent a primary source of morbidity in this population. While postural instability naturally worsens over time, a sudden cluster of falls over a week often stems from orthostatic hypotension. Studies show that roughly thirty-five percent of individuals with advanced Parkinson's suffer from this sudden drop in blood pressure upon standing. This cardiovascular autonomic dysfunction causes transient cerebral hypoperfusion, leading to dizziness, imbalance, and subsequent drops to the floor. As a result: adjusting blood pressure medications or increasing fluid and salt intake can rapidly mitigate the falling episodes, proving that the underlying neurological state has not fundamentally collapsed.
A Definitive Stance on Navigating Sudden Changes
We must stop viewing every sudden physical regression in Parkinson's disease as a final, catastrophic nail in the coffin. It is a dangerous medical error to confuse an acute, reversible systemic crisis with the immutable progression of neurodegeneration. When a patient collapses into immobility overnight, do not mourn a permanent loss of function; instead, hunt relentlessly for the hidden infection, the trapped medication, or the silent psychological stressor. Our clinical priority must pivot from passive acceptance to aggressive, investigative diagnostics. In short, the Parkinsonian brain is a highly sensitive seismograph, and a sudden spike in symptoms is merely the needle reacting to an external tremor, not the destruction of the instrument itself.