Beyond the Shake: The Neurological Root of Behavioral Shifts
Parkinson's disease is, at its core, a ruthless thief of dopamine, targeting the substantia nigra in the brain. But the thing is, dopamine isn't just about smooth muscle movement; it is the currency of our reward system, our motivation, and our impulse control. When 80% of dopamine-producing neurons die off, the brain's internal wiring sparks wildly. We are far from a simple mobility issue here. The resulting chemical drought triggers a cascade of psychological volatility that catches families entirely off guard.
The Dopamine Double-Edged Sword
Here is where it gets tricky. To treat the physical stiffness, neurologists prescribe dopamine agonists or Levodopa, which flood the brain with synthetic reward chemicals. It works wonders for the physical shuffle—until it overstimulates the mesolimbic pathway, the brain's hedonistic highway. Suddenly, a 65-year-old grandmother from Hamburg who never risked a single euro is secretly draining her retirement account on digital poker apps. Impulse Control Disorders (ICDs) affect up to 14% of patients on standard therapies, turning mild-mannered individuals into compulsive shoppers, hypersexual partners, or binge eaters. It is a devastating trade-off, and honestly, it’s unclear whether the disease or the cure causes more domestic wreckage.
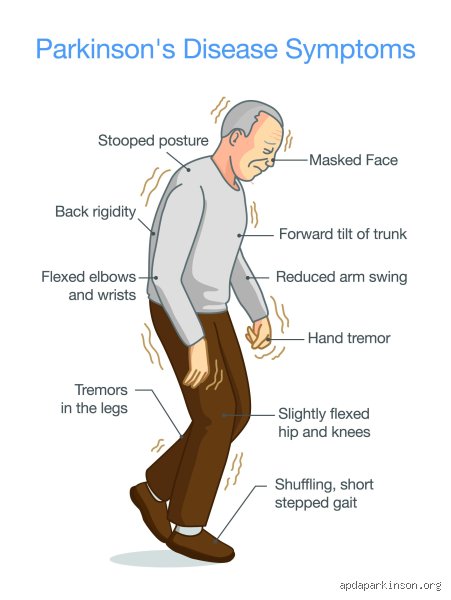
The Mask That Hides the Mind
But people don't think about this enough: the physical and the psychological are twisted together in agonizing ways. Take hypomimia, the medical term for the "Parkinson’s mask." Because facial muscles freeze, patients lose the ability to smile, frown, or flash a subtle look of surprise. Yet, observers routinely mistake this blank stare for apathy, depression, or intellectual decline. Imagine screaming internally with frustration while your face registers nothing but absolute, stony indifference to your spouse’s tears. That changes everything about how a family communicates, transforming dinner table conversations into minefields of unintended slights.
Nightmares in Motion: The Disruption of Sleep and Reality
If the daytime behaviors are jarring, the nighttime shifts are downright terrifying. What are the strange behaviors of Parkinson’s patients when the lights go out? They act out their most violent nightmares with startling physical force. In a healthy brain, REM sleep comes with a built-in safety switch—temporary muscle paralysis—so you don't actually punch the monster you are dreaming about. Except that in Parkinson’s, this switch fails spectacularly.
The Violence of REM Sleep Behavior Disorder
This glitch is known as REM Sleep Behavior Disorder (RBD), and it is a massive red flag, often predating the actual motor tremors by a decade or more. A study from the Mayo Clinic in 2023 confirmed that a staggering 50% of Parkinson’s patients suffer from this nocturnal disruption. They kick, thrash, swear, and shatter bedside lamps while sound asleep. I once spoke with a caregiver in Leeds whose husband nearly suffocated her because he dreamed he was wrestling a stray bear off their porch. It isn't aggression in the psychological sense—the person is completely unconscious—yet the physical danger to bed partners remains a silent, bruising crisis.
When Shadows Turn to Spiders
And then come the waking visions. As the disease creeps into the cortex, or as medication toxicity peaks, visual hallucinations become a vivid, everyday reality. These aren't abstract blobs of light; they are highly structured, distinct entities. Patients report seeing phantom children sitting quietly in the corner of the living room, or mechanical spiders crawling across the ceiling. What is fascinating—and deeply heartbreaking—is that early on, patients retain insight. They know the Victorian girl standing by the curtains isn't real, but that doesn't make the visual presence any less exhausting to endure.
The Obsessive Brain: Punding and the Trap of Repetition
Among the galaxy of quirky manifestations, few things baffle families quite like punding. This refers to a compulsive, entirely purposeless fascination with sorting, dismantling, or arranging objects. It is a behavior originally observed in chronic amphetamine users, which makes sense when you realize Parkinson’s drugs can overstimulate the brain in a identical fashion.
The Endless Sorting of Nothing
A patient might spend twelve consecutive hours arranging buttons by shade, taking apart lawnmowers without ever repairing them, or cataloging old receipts from 1994 until their fingers bleed. If you try to interrupt them? They react with intense anxiety or uncharacteristic flashes of rage. It is a pure, unadulterated dopamine loop. The brain gets hooked on the micro-reward of the repetitive action, completely overriding the basic human needs for food, hydration, or sleep. It looks like obsessive-compulsive disorder, but the underlying neurology is fundamentally distinct, driven by a medication-induced reward malfunction rather than classic anxiety.
Differentiating Parkinson’s Anomalies from Alzheimer’s and Lewy Body Dementia
When these bizarre actions surface, panic usually sets in, leading families to assume their loved one has rapidly slid into advanced Alzheimer’s disease. But drawing a sharp line between these conditions is vital because treating them requires radically different medical strategies.
The Timeline of Cognitive Decay
The core difference lies in the chronological sequence of symptoms. In Alzheimer’s, memory loss and spatial disorientation lead the march, while motor skills remain intact until the final stages. Parkinson’s reverses this script. The tremors and rigidity dominate for years before any cognitive unraveling begins. However, the waters get muddy when discussing Dementia with Lewy Bodies (DLB). In DLB, the strange behaviors, severe hallucinations, and cognitive fluctuations hit simultaneously with the motor symptoms, or even precede them. Experts disagree on whether Parkinson’s disease dementia and DLB are two distinct illnesses or merely different points on the exact same spectrum. Either way, misdiagnosing a Parkinson’s patient's behavioral quirks as standard Alzheimer's can lead to the prescription of typical antipsychotics—drugs that can fatally worsen Parkinsonian rigidity.
Common mistakes and misinterpretations surrounding Parkinsonian symptoms
Confusing dopamine-driven compulsions with moral failings
Families often watch in absolute horror as a previously frugal grandparent suddenly burns through an entire retirement account on digital poker or accumulates a garage full of useless gadgetry. What looks like a sudden, late-life character flaw is actually a biological hijacking. The culprit here is not a sudden lack of ethics, but rather the very medication prescribed to fix the motor deficit. Dopamine agonists, while brilliant at restoring fluid movement, frequently overstimulate the brain's reward pathways. This neurological short-circuit triggers profound impulse control disorders. It turns out that up to 14 percent of patients undergoing this specific therapy develop severe, compulsive behaviors. Recognizing this distinction shifts the family dynamic from anger to medical intervention, which explains why adjusting the pharmaceutical regimen usually halts the behavior entirely.
The trap of assuming cognitive decline equals Alzheimer’s disease
When an individual begins staring blankly into space or reporting that the living room curtains are transforming into predatory animals, observers instantly jump to the wrong conclusion. They assume a standard dementia pathway is unfolding. Except that the cognitive profile here is fundamentally different from other neurodegenerative conditions. Fluctuating attention spans and vivid visual hallucinations are distinct hallmark features of Parkinson's disease dementia and Lewy body spectrum disorders. The underlying pathology involves alpha-synuclein protein aggregates rather than amyloid plaques. Why does this nuance matter? Because treating these specific hallucinations with traditional antipsychotic medications can cause catastrophic, sometimes fatal, drops in motor function. Misidentifying these strange behaviors of Parkinson's patients leads directly to dangerous prescribing cascades that worsen the patient's physical stability.
The hidden reality of REM Sleep Behavior Disorder
When dreams turn physically violent
Have you ever had to dodge a full-force punch from your sleeping partner? For many caregivers, this is a terrifying weekly reality. During normal sleep, the brain stem paralyzes our muscles to keep us safe during vivid dreams. In this pathology, that safety switch fails completely. Patients physically act out their nightmares, which often involve defending themselves against vivid, imaginary attackers. They kick, thrash, yell, and dive out of bed. As a result: fractures, concussions, and severe bruises become routine household hazards. Strange behaviors of Parkinson's patients during the nocturnal hours are not just quirky anomalies; they are highly predictive. This specific sleep disorder frequently predates the characteristic motor tremors by more than a decade, serving as a loud, early warning siren from the central nervous system.
Expert management strategies for nocturnal safety
Addressing this nighttime turbulence requires moving far beyond basic sleep hygiene. Clinical experience dictates that the immediate physical environment must be drastically altered. We advise removing bedside tables with sharp edges, installing padded floor mats, and sometimes even placing the mattress directly on the floor. Low-dose clonazepam or high-dose melatonin can successfully dampen these motor outbursts by stabilizing the disrupted sleep architecture. Yet, we must admit the limits of current science, as these interventions merely suppress the symptoms rather than repairing the damaged brainstem nuclei. Let's be clear: a quiet night is the goal, but achieving it demands constant tracking of daytime medication wear-off effects as well.
Frequently Asked Questions
Why do some Parkinson's patients suddenly freeze while walking through doorways?
This baffling phenomenon is known as freezing of gait, a transient episode where a person's feet feel literally glued to the floor despite their intense desire to step forward. It is a complex episodic motor breakdown that occurs most frequently when navigating tight spaces, turning around, or approaching a visible threshold. Quantitative motion studies indicate that up to 60 percent of individuals in the advanced stages of the disease experience these abrupt motor blocks. The brain struggles to process the sudden change in visual information, which causes a temporary overload in the basal ganglia's motor planning loops. Utilizing external sensory cues, such as a laser pointer line or a rhythmic metronome beat, can effectively bypass this neurological roadblock and restart the walking sequence.
Can Parkinson's disease cause sudden, uncontrollable bursts of anger or emotional shifts?
Yes, profound mood lability and sudden behavioral shifts are directly tied to the neurodegenerative process itself. The disease systematically erodes not just dopamine pathways, but also serotonin and norepinephrine networks, which are the primary chemical systems responsible for stabilizing human emotion. Because these neurotransmitters are depleted, a patient might experience rapid swings from deep apathy to intense, unprovoked frustration over minor daily tasks. Unpredictable behavioral changes in Parkinson's disease are frequently exacerbated by the physical exhaustion of fighting motor symptoms all day. Caregivers should view these emotional outbursts as involuntary neurological storms rather than intentional hostility or a chosen psychological stance.
What causes the intense fixation on repetitive, meaningless tasks like sorting buttons?
This specific, repetitive behavior is clinically termed punding, a condition characterized by an intense fascination with purposeless activities like dismantling clocks, organizing papers, or meticulously sorting small objects for hours on end. It is a side effect tied closely to high doses of levodopa and dopamine replacement therapies, which over-saturate the ventral striatum. The patient feels a compulsive, rewarding urge to continue the repetitive activity, often becoming highly agitated if their focus is interrupted. Data shows this phenomenon affects approximately 1.4 to 14 percent of treated patients, depending heavily on the dosage levels and individual vulnerability. Managing this requires a delicate, expert reduction of dopaminergic medication without causing a total collapse of the patient's physical mobility.
An honest reckoning with the atypical realities of neurodegeneration
We need to stop pretending that Parkinson's disease is merely a matter of shaky hands and slow walking. The medical community and the public must confront the reality that the neuropsychiatric manifestations are often far more debilitating than the physical tremors. The issue remains that we are failing families if we only monitor their physical mobility scores during brief clinical visits. These complex cognitive disruptions and compulsive loops demand aggressive, open discussion and tailored pharmacological adjustments. It is time to dismantle the stigma surrounding these bizarre nocturnal and diurnal actions. Let's be clear: validating these unsettling changes as direct, physical brain injuries is the only compassionate path forward. Ultimate success in care management relies entirely on looking past the motor veneer to treat the whole, fractured neurological landscape.