The Illusion of a Uniform Clock: Defining Parkinsonian Progression
We love patterns. The human brain craves a neat, linear schedule, especially when confronting a neurodegenerative diagnosis. But Parkinson’s disease refuses to play along. When a patient sits in a neurology clinic at Johns Hopkins or the National Hospital for Neurology in London, they want a date. They want to know when the wheelchair arrives. The thing is, providing a single, universal expiration date on mobility is medically irresponsible because the underlying pathology operates on multiple, overlapping gears.
The Dopaminergic Tipping Point
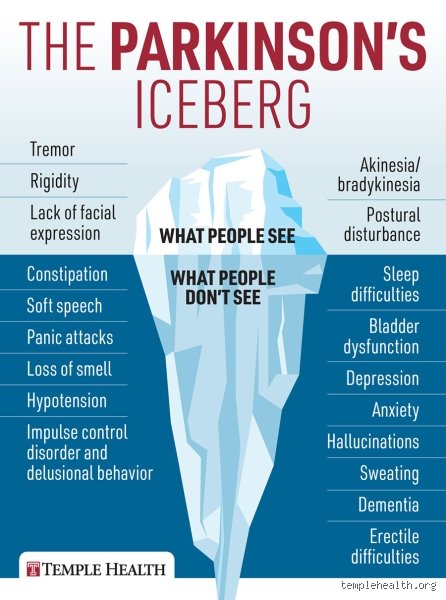
By the time that classic, resting pill-rolling tremor shows up in a thumb, the brain has already been losing ground for a long time. Specifically, about 60% to 80% of dopamine-producing neurons in the substantia nigra have already perished before the first clinical symptom emerges. This stealth phase—often called the prodromal period—can last for a decade, masquerading as stubborn constipation, shoulder stiffness, or a muted sense of smell. So, when we ask how fast the disease deteriorates, we are usually ignoring the massive, silent head start it already enjoyed. It feels sudden to the patient, yet the brain has been compensating masterfully for years until it simply cannot anymore.
Why the Term "Staging" Misleads Patients
Neurologists rely on the Hoehn and Yahr scale, a framework tracking progression from Stage 1 (unilateral involvement) to Stage 5 (confinement to bed or wheelchair). But people don't think about this enough: these stages are not equal blocks of time. A person might hover at Stage 2 for twelve years, then transition to Stage 4 in twenty-four months due to a severe urinary tract infection or a broken hip. It is a staircase with steps of unpredictable, fluctuating heights, not a smooth ramp. I am firmly convinced that viewing Parkinson's through a rigid chronological lens causes more psychological harm than clinical utility.
The Biological Acceleraetors: What Actually Speeds Up the Decline?
If the baseline rate of deterioration is a slow burn, what throws gasoline on the fire? The answers lie within genetic architecture and cellular trash management.
Alpha-Synuclein Proteotoxicity and the Brain's Garbage Disposal
The core villain in this story is a misfolded protein called alpha-synuclein, which aggregates into toxic clumps known as Lewy bodies. Think of it as a plumbing crisis in the neocortex. In rapidly progressing phenotypes, these proteins spread through the brain's interconnected networks like a wildfire through dry brush, moving from the brainstem up to the cerebral cortex with terrifying efficiency. Why does this happen faster in some? It usually comes down to the failure of the lysosomal pathway—the cellular garbage disposal. When mutations in the GBA1 gene are present, which happens in roughly 5% to 10% of cases, the disposal system breaks down completely, causing alpha-synuclein to accumulate at double the speed of standard idiopathic Parkinson's.
The Double Whammy of Age and Vascular Burden
Age at onset changes everything. If you are diagnosed at age 45—young-onset Parkinson’s disease—your brain typically possesses a reservoir of neuroplasticity that fights back, keeping cognitive decline at bay for decades. Contrast this with a diagnosis at age 78. In older cohorts, the disease frequently marches at a brisker clip because the aging brain is already battling microvascular white matter disease. Data from a landmark 2018 study published in Frontiers in Neurology revealed that patients diagnosed after age 75 manifested severe gait disturbances and cognitive impairment up to three times faster than their younger counterparts. It is an unfair math equation where pre-existing systemic wear-and-tear accelerates the neurodegenerative clock.
Phenotypic Profiles: The Tremor-Dominant vs. PIGD Divide
To predict velocity, we must look at the specific flavor of Parkinson’s a person presents with, because the clinical manifestations diverge sharply right at the starting line.
The Tremor-Dominant Safe Haven
Here is where we encounter a strange paradox that contradicts conventional wisdom: having a prominent, highly visible shaking hand is actually good news. The Tremor-Dominant (TD) phenotype is historically associated with a significantly slower rate of deterioration. Patients with loud, persistent tremors often experience a benign course where dementia risks remain low for up to fifteen years post-diagnosis. They shake, yes, but their core stability, posture, and mental clarity remain largely intact, allowing them to adapt, modify their environments, and continue working or traveling long after their peers have faced significant mobility milestones.
The Ominous Shift to Postural Instability and Gait Disorder (PIGD)
Where it gets tricky is the other major subtype: Postural Instability and Gait Disorder, or PIGD. Instead of tremors, these individuals present early on with a stiff, shuffling walk, frequent balance losses, and the frightening phenomenon of "freezing" mid-step. The prognosis here is markedly different. PIGD variants deteriorate toward requiring assistive devices much faster, with up to 45% of patients experiencing significant falls within the first five years of symptom onset. The degenerative process in PIGD isn't confined neatly to dopamine pathways; it aggressively invades cholinergic systems, which explains why balance and memory degrade in tandem.
The Great Diagnostic Mirage: Parkinson’s vs. The "Plus" Syndromes
Sometimes, a trajectory looks terrifyingly fast because the diagnosis was wrong from the beginning. Honestly, it's unclear in the first twenty-four months exactly what you are dealing with, even for seasoned movement disorder specialists.
The Ghost of Multiple System Atrophy
When a patient deteriorates from a minor limp to being completely wheelchair-bound within thirty-six months, the seasoned clinician stops thinking about classic Parkinson’s and starts suspecting atypical parkinsonism. The most aggressive mimic is Multiple System Atrophy (MSA). In MSA, the autonomic nervous system collapses early, causing blood pressure to plummet upon standing, alongside severe bladder dysfunction. While a classic Parkinson's patient might expect a normal or near-normal life expectancy, the median survival for MSA is a brutal 6 to 9 years from onset. It is an entirely different beast wearing a familiar mask.
Progressive Supranuclear Palsy and the Downward Gaze
Another high-speed derailment occurs with Progressive Supranuclear Palsy (PSP). Except that instead of just slowness, PSP damages the brainstem nuclei controlling eye movement. If a patient comes into a clinic in Boston or Tokyo complaining that they keep falling down stairs because they literally cannot look down, the clock resets. PSP progresses relentlessly, with severe dysphagia and speech loss occurring within 3 to 5 years. Distinguishing these syndromes early is paramount for management, yet we are far from having a simple, definitive blood test to sort them out on day one.
Common mistakes and misconceptions about progression
People often assume that a Parkinson's diagnosis equals an immediate, linear slide toward immobility. It does not. The trajectory is rarely a straight line, which explains why mapping out exactly how quickly does Parkinson's deteriorate baffles even experienced neurologists. Families frequently expect a predictable timeline, looking at Hoehn and Yahr scales as if they were rigid calendar appointments. They are not. You might stay at stage two for a decade, then shift unexpectedly after a severe urinary tract infection or a period of intense psychological stress.
The linear downfall fallacy
Let's be clear: degeneration is a jagged staircase, not a smooth ramp. A common blunder is assuming that today's symptom acceleration dictates next year's velocity. It is entirely possible to experience a aggressive flare-up of bradykinesia over six months, only to have the disease plateau for the next five years. Dopaminergic neurons do not die on a synchronized schedule. Because of this erratic cellular decay, evaluating the speed of decline based on a single bad month is an exercise in futility. Progression rates in Parkinson's disease remain fiercely idiosyncratic.
Equating tremor with rapid decline
Does a violent tremor mean the end is nigh? Paradoxically, the opposite is frequently true. Patients presenting with prominent resting tremors often experience a significantly slower rate of motor decay compared to those with the postural instability gait difficulty subtype. But the general public sees a shaking hand and assumes the brain is dismantling itself at warp speed. The issue remains that the most visually dramatic symptom is frequently the least predictive of long-term cognitive or functional disability. It is the silent, non-motor symptoms like orthostatic hypotension that actually signal a more aggressive course.
The silent accelerator: Neuroinflammation and sleep
We spent decades obsessing exclusively over alpha-synuclein aggregates. Except that we ignored the campfire raging around them. Microglial activation—the brain's immune response gone rogue—acts as a massive accelerant on the disease's timeline. When these cells remain perpetually angry, they secrete pro-inflammatory cytokines that destroy neighboring healthy tissue, effectively answering the burning question of how fast does Parkinson's advance with an unwelcome boost in speed.
The glymphatic failure link
Have you ever considered how your brain dumps its trash? This happens via the glymphatic system, a microscopic plumbing network that operates almost entirely while you are in deep REM sleep. When Parkinson's disrupts sleep architecture—which it does in up to 80% of patients—this sanitation system breaks down. The result: toxic proteins accumulate faster because the nightly rinse cycle is skipped. Improving sleep hygiene is not a luxury; it is a direct intervention to slow down the rate of neurological decline.
Frequently Asked Questions
Can you slow down how quickly Parkinson's deteriorates?
Yes, intensive physical intervention directly alters the neuroplastic capabilities of the surviving dopaminergic pathways. Clinical data from the landmark SPARX trial demonstrated that high-intensity treadmill exercise at 80% to 85% of maximum heart rate effectively neutralized motor symptom progression over a six-month period compared to sedentary controls. The problem is that regular, leisurely walking is simply insufficient to trigger the release of brain-derived neurotrophic factor. You must push the cardiovascular system to its safe limits to achieve true neuroprotection. As a result: sweat becomes just as mandatory as your carbidopa-levodopa prescription.
Does age at diagnosis change how fast Parkinson's advances?
Age is arguably the most powerful predictor of the disease's velocity. Individuals diagnosed with young-onset Parkinson's disease, typically under the age of 50, usually experience a much more prolonged, gradual course spanning several decades. Conversely, late-onset patients diagnosed after age 75 frequently exhibit a accelerated trajectory, often developing cognitive impairment or dysphagia within 3 to 5 years of symptom onset. This discrepancy exists because older brains possess less cognitive reserve and often harbor concurrent vascular pathology. (And let's not forget that older systems tolerate high doses of dopaminergic medications much less effectively.)
How quickly does Parkinson's deteriorate to dementia?
The timeline for cognitive decline is highly variable, though long-term longitudinal studies paint a sobering picture. Data indicates that approximately 40% of patients will develop Parkinson's disease dementia within 10 years of their initial diagnosis, a number that climbs to nearly 80% for those who survive 20 years with the condition. Early emergence of visual hallucinations or severe executive dysfunction is a strong statistical indicator that cognitive decline will proceed rapidly. Yet, a fortunate cohort of patients retains excellent intellectual clarity throughout their entire disease journey, highlighting the danger of universal assumptions.
A definitive perspective on the timeline
We must stop treating Parkinson's disease as a uniform death march with a fixed expiration date. The medical community often cloaks its prognosis in vague generalities, but the stark reality is that your lifestyle, genetic architecture, and vascular health dictate the clock's speed. Standing idly by while waiting for a pharmaceutical silver bullet to halt the speed of Parkinson's degeneration is a losing strategy. Passive patients decline rapidly, whereas aggressive, proactive individuals who weaponize high-intensity exercise and meticulous sleep management frequently bend the progression curve in their favor. The ultimate velocity of this disease is not entirely written in your DNA. Take control of the variables you can manipulate, because the brain will not negotiate with hesitation.