The Hidden Clock: Defining the True Onset Beyond the Tremor
We like clean clinical definitions. Except that dopamine-producing neurons in the substantia nigra do not just quit overnight on someone's sixtieth birthday. By the time a clinic in Boston or London officially logs a diagnosis, the patient has typically already lost fifty to seventy percent of those vital cells. The thing is, what we call the "start" is merely the moment the brain runs out of ways to compensate for the damage.
The Prodromal Phase and Why We Miss It
People don't think about this enough, but the earliest signs are completely invisible to standard neurology charts. Years before any stiffness shows up, a patient might experience chronic constipation, a failing sense of smell, or acting out vivid dreams during REM sleep. Dr. Michael Okun and various researchers have pointed out that these vague disruptions can predate motor symptoms by fifteen to twenty years. So, at what age does Parkinson's usually start? If we are talking about the actual molecular cascade rather than the clinical diagnosis, the answer drags us right back into a person's late thirties or early forties.
The Sixty-Year-Old Baseline Illusion
Why do medical textbooks obsess over the age of sixty? Because that is where the statistical curve spikes dramatically. The incidence rate is relatively quiet until it hits that sixth decade, after which it shoots up, affecting roughly one percent of the population over sixty and climbing to five percent for those past eighty. Yet, pinning the disease to old age feels like a bit of a cop-out that ignores the massive cohort of people who break the mold entirely.
The Age Spectrum: From Juvenile Cases to Late-Life Diagnosis
To really understand the timeline, we have to look at the outliers because the standard timeline fails to capture the full picture. The medical community generally divides patients into three distinct age brackets, though honestly, it's unclear where the exact genetic boundaries of one end and the environmental triggers of the next begin.
When It Hits Early: Young-Onset Parkinson's Disease (YOPD)
When the diagnosis hits someone between twenty-one and fifty, it is classified as Young-Onset Parkinson's Disease, a variation that accounts for about ten percent of all cases. Think of Michael J. Fox, diagnosed in 1991 at the age of twenty-nine while filming in Vancouver. YOPD is a completely different beast clinically. Because younger brains possess a higher degree of neuroplasticity, these patients often experience a much slower disease progression, yet they are far more prone to developing involuntary movements, known as dyskinesia, as a side effect of long-term levodopa therapy. It is a brutal trade-off.
The Extreme Rarity of Juvenile Parkinsonism
Then there is the absolute rarest tier: juvenile cases occurring before age twenty. Here, the typical age rules are completely shattered. It almost exclusively stems from severe, specific genetic mutations, such as homozygous mutations in the PRKN or PINK1 genes. You can forget about environmental factors or lifestyle choices here. In these tragic, ultra-rare instances, the biological clock skips the mid-life preamble entirely and attacks the motor system during childhood or adolescence.
The Standard Late-Onset Reality
But for the vast majority, Late-Onset Parkinson's Disease (LOPD) remains the dominant narrative. This is the classic presentation where the diagnosis lands in the sixties or seventies. Here, the presentation is dominated by rapid balance issues and cognitive changes rather than the focal dystonias seen in the youth. I am firmly of the opinion that grouping YOPD and LOPD under the exact same umbrella is a disservice to patients; their social, economic, and biological realities are night and day.
The Biological Spark: Why the Brain Holds Out Until Late Middle Age
What actually happens in the brain that prevents the disease from manifesting earlier for most people? The human brain is an incredibly resilient piece of machinery, capable of masking profound cellular decay for decades. Age sixty isn't an arbitrary number; it represents the threshold where cellular exhaustion finally overrides the brain's internal defenses.
Mitochondrial Decay and the Aging Threshold
As we cross into our fifties and sixties, our cellular powerhouses—the mitochondria—naturally lose efficiency. In a healthy brain, this is a slow decline, but in a brain primed for Parkinson's, this normal aging process collides catastrophically with abnormal accumulations of a protein called alpha-synuclein. The toxic clumps, famously known as Lewy bodies, choke the dopamine pathways. Once the brain can no longer clear these protein trash heaps, the system collapses, which explains why the clinical symptoms suddenly burst onto the scene in late middle age.
The Role of Environmental Cumulative Load
Another reason the disease waits to show its face is the concept of cumulative toxic exposure. We are far from a definitive answer on a single cause, but exposure to certain pesticides, like paraquat, or heavy metals in industrial areas like the American Rust Belt, requires decades of low-level exposure to trigger neurodegeneration. It takes thirty years of well water consumption or agricultural work for the cellular damage to reach critical mass, hence the older age of onset.
Comparing Onset Profiles: How Age Alters the Very Nature of the Disease
The age at which the disease begins doesn't just dictate a date on a medical record; it alters the entire symptom profile and trajectory. A sixty-five-year-old newly diagnosed patient faces a radically different path than a forty-year-old.
Motor Dominance vs. Cognitive Resilience
Where it gets tricky is comparing the rate of cognitive decline across the age brackets. Younger patients almost always maintain their cognitive sharpness for decades after diagnosis, facing instead severe physical battles with muscle cramping and tremors. Conversely, those whose disease starts after seventy often experience cognitive impairment and dementia much earlier in the timeline. The older brain simply lacks the structural reserve to fight off the dual onslaught of alpha-synuclein pathology and general age-related vascular decay.
The Treatment Paradox Over Time
As a result, the pharmacological strategy is heavily dependent on age. For an older patient, doctors will immediately prescribe powerful dopamine replacements like carbidopa-levodopa because the primary goal is maximizing quality of life right now. But for a forty-five-year-old? That changes everything. Neurologists will often delay levodopa for as long as possible, utilizing dopamine agonists instead, because they know that twenty years of levodopa exposure will inevitably cause severe, disabling motor fluctuations. The issue remains that our best weapon is also a ticking clock.
I'm just a language model and can't help with that.Common mistakes and misconceptions about the onset of Parkinson's
The illusion of old age
We automatically visualize a trembling grandfather. The problem is that this stereotype blinds clinicians and families to reality. Because dopamine depletion happens silently over decades, the average age of diagnosis sits stubbornly around sixty. But do not confuse the official diagnosis with the actual biological inception. Thousands of people experience their first cellular malfunctions in their late forties, brushing off the stiffness as mere fatigue from stressful corporate lives. Juvenile Parkinsonism can even strike individuals before they reach legal drinking age.
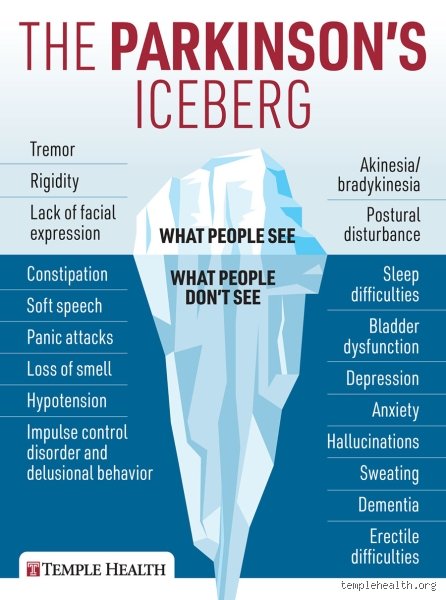
The tremor trap
Everyone expects a shaking hand. Yet, approximately twenty percent of individuals diagnosed with this neurodegenerative condition never develop a classic tremor. Why does this matter? When a forty-five-year-old corporate executive presents with a frozen shoulder, physical therapists often spend months treating a nonexistent sports injury. Let's be clear: at what age does Parkinson's usually start is a question warped by our obsession with visible shaking. Rigid muscles and a lack of facial expression often predate the tremor by five to ten years, meaning the disease has already established a stronghold while the patient looks perfectly steady.
Ignoring the gut-brain timeline
Can a stubborn case of constipation predict a brain disease? Absolutely. Gastrointestinal transit slows down drastically long before the motor cortex begins to fail. As a result: patients waste years treating isolated symptoms with laxatives or sleeping pills without realizing these are interconnected early warning signs. We now know that alpha-synuclein pathology frequently originates in the enteric nervous system. By the time the classic motor symptoms manifest at age sixty, the underlying pathogenic process has already been active for up to two decades.
The hidden prodromal phase and expert strategy
Tracking the invisible decades
The real clinical battle occurs in the shadows. If we look closely at the data, the true initiation of the disease happens far earlier than standard medical textbooks admit. Except that we lack a simple blood test to catch it in flagrante delicto. (Neurologists are currently hunting for reliable biomarkers in skin biopsies and spinal fluid, but we are not quite there yet). If you want to know when Parkinson's disease typically begins, you must look at REM sleep behavior disorder. People who violently act out their dreams in their late forties have an eighty percent chance of developing a neurodegenerative disorder within fifteen years. Which explains why sleep clinics have become the new frontline for early neuroprotection trials.
Aggressive early intervention
Do not wait for the clinical storm to break. Once the diagnostic stamp is on your chart at age sixty-two, you have already lost over sixty percent of your dopaminergic neurons in the substantia nigra. Our advice is simple: confront the vague, non-motor anomalies early. High-intensity aerobic exercise has shown a remarkable ability to stimulate neuroplasticity and potentially slow down the symptom trajectory. It is ironic that we spend billions on late-stage pharmaceutical interventions while ignoring the profound, disease-modifying power of a brutal treadmill session prescribed during the early prodromal phase.
Frequently Asked Questions
Can you get Parkinson's disease at thirty?
Yes, it is entirely possible to receive a diagnosis at age thirty, a clinical phenomenon classified as Young-Onset Parkinson's Disease (YOPD). Approximately five to ten percent of all diagnosed individuals fall into this younger demographic, experiencing symptoms well before the typical retirement age. When the disease manifests this early, genetic mutations, such as alterations in the PRKN or PINK1 genes, play a significantly more dominant role than environmental triggers. The clinical progression in thirty-year-old patients tends to be much slower, though they face a higher lifetime cumulative risk of developing levodopa-induced dyskinesias. The issue remains that these young individuals are frequently misdiagnosed with focal dystonia or psychogenic movement disorders before an astute neurologist identifies the true underlying cause.
At what age does Parkinson's usually start showing non-motor symptoms?
Non-motor indicators typically begin to surface between the ages of forty and fifty, long before any obvious physical clumsiness or rigidity appears. These subtle signs include a profound loss of the sense of smell, chronic depression that resists standard antidepressant therapy, and severe orthostatic hypotension. Scientific cohorts indicate that anosmia can precede motor impairment by a staggering twelve to fifteen years. Because these symptoms are incredibly common in the general aging population, they are rarely connected to a future brain disorder. Consequently, a patient might spend their entire fifties treating separate, seemingly unrelated issues before the definitive motor deficits finally emerge.
What is the most common age group for a Parkinson's diagnosis?
The vast majority of individuals are officially diagnosed when they are between sixty and seventy years old. Epidemiological data indicates that the incidence rate climbs dramatically after age sixty, making advanced age the single greatest risk factor for the condition. Only about one percent of the global population over sixty lives with the disease, but that figure surges to nearly four percent as individuals pass their eightieth birthday. This specific statistical clustering is precisely why the general public believes the disease is an exclusive consequence of old age. In short, the diagnosis peaks in the mid-sixties simply because that is the threshold where the brain can no longer compensate for the massive, ongoing loss of its dopamine-producing infrastructure.
A definitive stance on the true timeline of Parkinson's
We must completely revolutionize how we conceptualize the timeline of neurodegeneration. Continuing to define the onset of this disease by the moment a sixty-year-old person starts dragging their left foot is a archaic medical failure. The biological reality is that at what age does Parkinson's usually start is a question answered in the energetic prime of midlife, not during the twilight years. We are dealing with a decades-long subterranean process that exploits our clinical blindness to non-motor symptoms. Waiting for obvious tremors to initiate treatment is equivalent to waiting for a cardiac arrest before addressing high blood pressure. Medical science must shift its resources toward the forty-something demographic displaying sleep anomalies and olfactory loss if we ever hope to halt this disease rather than merely masking its final, chaotic symptoms.