Decoding the True Timeline of Neurodegeneration: When Does Parkinson's Disease Actually Start?
To understand the timeline, we have to look past the physical shaking. The reality is that the brain is a master of compensation, masking the destruction of dopamine-producing neurons in the substantia nigra until nearly 60% to 80% of them are already gone. Think of it like a massive retaining wall that secretly rots from the inside out; it looks perfectly stable to passersby until a sudden summer storm washes the whole structure down the hillside. By the time a patient in London or New York walks into a clinic with a stiff wrist, the disease is already an old tenant. Neurological onset vs clinical diagnosis are two entirely different beasts. Because of this lag, the medical community has historically focused on the wrong end of the timeline.
The Substantia Nigra and the 60-Percent Tipping Point
Where it gets tricky is the cellular math. The human brain contains a dense cluster of melanin-rich cells that produce dopamine, a neurotransmitter that acts like grease in the gears of our motor system. But here is the thing: we lose these cells naturally as we age, roughly 5% per decade. In a patient destined for a Parkinson's diagnosis, this attrition rate skyrockets. Yet, the body shows no outward signs of distress during this initial phase. Why? Because the remaining neurons simply work overtime, stretching their axons to handle the extra workload until they hit that catastrophic 60% loss threshold.
Alpha-Synuclein Infiltration: The Decade-Long Pre-Motor Phase
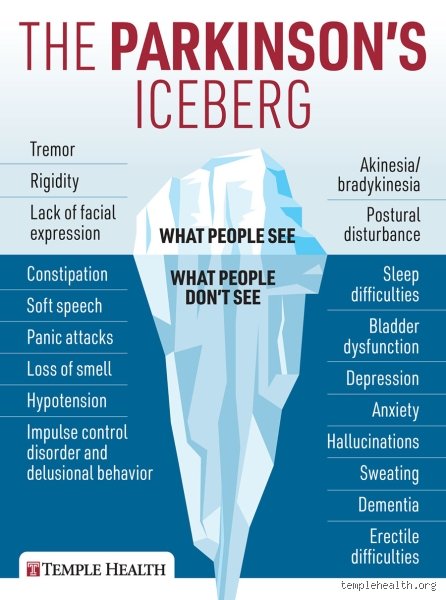
Long before the motor symptoms break through the surface, a rogue protein called alpha-synuclein begins to misfold and clump together into toxic aggregates known as Lewy bodies. It doesn't start in the motor centers either. German neuroanatomist Heiko Braak revolutionized our understanding in 2003 by showing that these proteins actually creep upward from the enteric nervous system—the "gut brain"—and the olfactory bulb. This explains why a future patient might suffer from severe, intractable constipation or lose their sense of smell in their late thirties. People don't think about this enough, but a dull nose in 2015 could be the first domino falling for a diagnosis in 2035.
The Statistical Sweet Spot: Breaking Down the Average Age of Parkinson's Diagnosis
If you look at the raw numbers from organizations like the Michael J. Fox Foundation, the average age of Parkinson's diagnosis sits stubbornly between 60 and 62 years old. But averages are dangerous things that smooth over a chaotic reality. It is a bell curve with jagged edges. While the vast majority of cases populate the zone between 55 and 75, there is a terrifyingly large cohort of people who fall outside these neat boundaries. Late-onset Parkinson's disease (LOPD) strikes those past 75, often presenting with rapid cognitive decline that looks suspiciously like Alzheimer's, which complicates things immensely. Honestly, it's unclear whether old age simply makes the brain more vulnerable to the protein pathology or if we are looking at a completely different subtype of the illness.
The Geographic and Demographic Shifting Lines
The numbers change depending on where you look on the map. A comprehensive 2022 epidemiological study published in The Lancet revealed that industrial corridors in the American Midwest—places like Ohio and Pennsylvania—show a slightly lower average age of onset than rural areas in western Europe. Why? Environmental triggers like paraquat, a widely used herbicide, and trichloroethylene (TCE), an industrial solvent found in groundwater, seem to accelerate the biological clock. A factory worker in Cleveland exposed to degreasing agents might see their first symptoms at 54, while a schoolteacher in sunny southern France might coast until 67 before the first shuffle appears.
The Illusion of the Senior Citizen Disease
We've built a collective cultural myth around the trembling elderly grandparent. But that image does a massive disservice to the thousands of individuals who don't fit the script. When we look at global prevalence data, roughly 1% of the population over 60 has the condition, but that number jumps to nearly 3% for those past 80. Yet, focusing exclusively on these senior statistics creates a blind spot for primary care physicians. A 42-year-old woman complaining of a frozen shoulder and profound fatigue is often sent to physical therapy for months, if not years, because her doctor thinks she is far too young for a neurodegenerative disease. We are far from a perfect diagnostic system.
When the Clock Speeds Up: Understanding Young-Onset Parkinson's Disease (YOPD)
But what happens when the timeline collapses completely? When a person is diagnosed before the age of 50, the medical community categorizes it as Young-Onset Parkinson's Disease (YOPD). This isn't just a rare anomaly; it accounts for roughly 5% to 10% of the entire Parkinson's population. I have seen vibrant, thirty-something professionals—marathon runners, software engineers, young mothers—suddenly forced to navigate a medical landscape designed almost exclusively for retirees. The clinical progression here is fundamentally different. While older patients often struggle with early balance issues and cognitive clouding, younger patients tend to experience severe involuntary muscle contractions, known as dystonia, and a much higher rate of depression.
The Genetic Trapdoors: PRKN, PINK1, and LRRK2 Mutations
In the older demographic, genetics is usually a background player, a vague suggestion of risk. In young-onset cases, however, DNA often holds the smoking gun. Mutations in genes like PRKN (Parkin) and PINK1 are notorious for triggering early-onset forms of the disease, frequently showing autosomal recessive inheritance patterns that can skip generations only to devastate a family in their thirty-first year. Then there is the LRRK2 gene mutation, particularly prevalent among Ashkenazi Jewish and North African Berber populations, which acts like a ticking biological time bomb that can detonate at 45 or 85—the penetrance is maddeningly unpredictable. If you inherit the bad copy, your cellular garbage disposal system fails, mitochondria burn out prematurely, and the substantia nigra undergoes a quiet, early massacre.
The Heavy Burden of the Early-Onset Professional
The societal cost of YOPD is immense. An individual diagnosed at 68 has often reached retirement, their children are grown, and their life insurance is settled. A person diagnosed at 38 is at the absolute peak of their earning potential, likely carrying a massive mortgage, and trying to raise toddlers. The psychological toll of watching your body slowly rebel while you are supposed to be in your prime is a distinct brand of hell that older patients rarely have to confront in the same way. Furthermore, younger brains are far more prone to levodopa-induced dyskinesias—those loose, writhing movements that look like a frantic dance—meaning the very medication that restores their mobility eventually creates its own chaotic side effects.
Age vs. Mimics: How Early Symptoms Are Frequently Misdiagnosed Across Generations
The issue remains that Parkinson's is a diagnostic chameleon. Because there is no simple blood test to confirm its presence, clinicians must rely on a clinical exam, observing the patient's gait, facial expression, and finger-tapping speed. Except that these symptoms look like a dozen other things depending on how old the patient is. A 70-year-old with a slow walk is dismissed as "just getting old," while a 40-year-old with a slight tremor is told they drink too much coffee or are suffering from generalized anxiety disorder brought on by workplace stress. The age of the patient acts like a distorting lens for the clinician, hiding the true pathology behind a wall of demographic assumptions.
The Essential Tremor Confusion in Younger Adults
The most common diagnostic pitfall is essential tremor (ET), a neurological condition that is actually eight times more common than Parkinson's. How do you tell them apart? An essential tremor is an action tremor; it shows up when you try to use your hands, like holding a teacup or signing a check at a bank in Boston. A Parkinson's tremor is a resting tremor, appearing when the hands are relaxed in the lap, resembling a rhythmic "pill-rolling" motion. Yet, in a 45-year-old patient, many hurried general practitioners see a shaking hand and immediately write a prescription for beta-blockers, assuming it's ET, which explains why the average journey from first symptom to accurate Parkinson's diagnosis for younger folks takes nearly three years.
Normal Pressure Hydrocephalus and Vascular Mimics in the Elderly
At the other end of the age spectrum, the waters are just as muddy. Elderly patients often exhibit a "magnetic gait"—where their feet seem glued to the floor—that mirrors Parkinson's perfectly. But this can actually be caused by Normal Pressure Hydrocephalus (NPH), an accumulation of cerebrospinal fluid in the brain's ventricles, or by a series of silent, microscopic strokes in the white matter, known as vascular parkinsonism. Treat NPH with a surgical shunt, and the patient might walk normally again; mistake it for classic Parkinson's, load them up with dopamine agonists, and you will achieve nothing but severe hallucinations and a plummeting blood pressure. It is a high-stakes guessing game where age can easily trick even seasoned doctors into choosing the wrong therapeutic path.
Common Mistakes and Misconceptions About Parkinsonian Onset
The Old Person's Disease Trap
Most folks picture a frail octogenarian when they think of tremor-dominant neurological conditions. This is a massive blind spot. While the median age for a diagnosis hovers stubbornly around sixty-five, this statistical average acts like a thick fog obscuring a more complex reality. The problem is that assuming youth equals immunity delays critical medical interventions. Early-onset cases account for roughly 10% of all diagnoses, hitting individuals well before their fiftieth birthday. When you are forty, a stiff shoulder looks like a sports injury, not a dopamine shortage. Except that it often is the first quiet signal of a changing brain.
Chasing the Tremor Mirage
Everyone looks for the shake. Yet, focusing exclusively on resting tremors means missing the forest for the trees. Did you know that up to 25% of patients never experience a prominent tremor at any stage of their illness? Instead, they battle rigid muscles, slow movement, or unexplained clumsiness. Because society views shaking as the universal benchmark for when Parkinson's usually begins, these non-tremor symptoms get brushed off as stress or poor posture. Let's be clear: waiting for a trembling hand to appear before seeking a neurologist is a recipe for lost time.
Conflating Biological Onset with the Diagnosis Date
Here is a frustrating truth. The day a doctor signs your medical chart is not the day the disease started. The underlying neurodegenerative process actually kicks off decades before any visible motor symptoms emerge. By the time a clinical examination confirms bradykinesia, the brain has already lost an estimated 60% to 80% of its dopamine-producing neurons in the substantia nigra. Why do we keep treating the diagnostic date as the actual starting gun? It is an optical illusion that warps our understanding of the true timeline.
The Hidden Premotor Phase: An Expert's Perspective
The Decades-Long Silent Countdown
If you want to know at what age does Parkinson's usually begin, you have to look into the gut and the dream world. Decades before the motor system falters, subtle, seemingly unrelated disruptions manifest. Chronic, intractable constipation often plagues patients thirty years before a diagnosis. Another eerie harbinger is REM sleep behavior disorder, where people physically enact violent dreams because their brainstem fails to paralyze their muscles. Research indicates that up to 80% of individuals with this specific sleep pathology will eventually develop a synucleinopathy. The issue remains that we rarely connect these disparate dots until the motor system collapses.
The Olfactory Warning Bell
Have you ever suddenly lost your sense of smell without a stuffy nose? Hyposmia is one of the earliest signs that something is amiss in the central nervous system. This olfactory decline typically precedes motor dysfunction by at least four to five years. (Neurologists often joke that a scratch-and-sniff test is cheaper than a multi-thousand-dollar DaTscan, though it is far less definitive). As a result: we must train primary care physicians to view sudden, unexplained scent loss in fifty-year-olds with a much higher degree of suspicion rather than chalking it up to normal aging.
Frequently Asked Questions
Can you get Parkinson's in your 20s or 30s?
Yes, though it remains an exceedingly rare medical phenomenon. When the condition strikes before age forty, it is classified as Young-Onset Parkinson's Disease (YOPD). Statistics show that this specific demographic comprises less than 5% of the total patient population globally. In these unusually young individuals, genetic mutations, such as variants in the PRKN or PINK1 genes, play a significantly more dominant role than environmental factors. Treatment paths for these younger patients differ wildly from older cohorts, primarily because their brains are more susceptible to long-term levodopa-induced dyskinesias.
At what age does Parkinson's usually begin to show different symptoms between genders?
Gender-based symptomatic differences generally become apparent around the typical onset age of sixty. Men are diagnosed at a rate roughly 1.5 times higher than women, a gap that scientists believe may be linked to the protective effects of estrogen on dopamine neurons. When women do present with the condition, they frequently report higher levels of pain and postural instability rather than severe tremors. Conversely, male patients tend to exhibit greater rigidity and cognitive decline earlier in their disease progression. This divergence suggests that biological sex influences the vulnerability of specific neural pathways as we age.
Does a family history mean you will get it earlier?
Having a first-degree relative with the condition elevates your risk, but it does not automatically guarantee an earlier onset date. Roughly 15% of patients have a known family history of the disease, pointing to an intricate interplay between genetic predisposition and environmental triggers. Certain high-penetrance genetic mutations, like LRRK2 or GBA, can shift the chronological timeline, causing symptoms to manifest a few years earlier than the national average. But possession of these genes is not a absolute prophecy. Many individuals carrying these mutated alleles live well into their eighties without ever developing a single motor deficit.
A Call to Redefine the Timeline
We need to stop treating this disease as a sudden retirement-age catastrophe. The current medical framework relies on an outdated, reactive model that waits for a patient to start shaking before acting. This approach is fundamentally flawed because it ignores the twenty-year prodromal window where neuroprotection might actually stand a chance. We must aggressively shift funding and diagnostic protocols toward identifying the very earliest cellular shifts. Expecting a cure while ignoring the silent decades of early neurodegeneration is a fantasy. In short, the true battle against this condition must be fought when the brain is still seemingly healthy, not when the damage is already set in stone.