The evolution of emergency triage and why the order matters
We used to live in a simpler medical world where the classic ABC protocol reigned supreme. For decades, the American Heart Association and various international bodies drummed the Airway-Breathing-Circulation mantra into the heads of every paramedic, nurse, and battlefield medic. It made sense on paper. Yet, battlefield data from the Joint Trauma System during the early 2000s—specifically analyzing casualties in Iraq and Afghanistan—revealed a glaring, fatal flaw in this philosophy because exsanguination from massive arterial wounds was killing soldiers before anyone could even look at their mouth. That changes everything.
From ABC to March: The shifting paradigm of trauma response
Imagine dealing with an arterial spurt while trying to position a jaw-thrust maneuver. It is an exercise in futility. Consequently, the Committee on Tactical Combat Casualty Care spearheaded a massive structural overhaul in 1996, which eventually trickled down to civilian medicine, permanently altering our understanding of what is the correct order for primary assessment. The issue remains that civilian adaptation is notoriously slow, and even today, you will find legacy training programs teaching outdated techniques. Honestly, it is unclear why some institutions resist the shift, except that old habits die hard in bureaucratic medical boards.
The psychological anchor of a standardized clinical sequence
When adrenaline floods your system during an active code or a severe trauma call, your prefrontal cortex essentially goes offline. You do not think; you react. Having a rigid, immutable sequence prevents cognitive overload and stops what psychologists call tunnel vision, ensuring that a practitioner does not spend ten minutes splinting a fractured tibia while the patient quietly suffocates from a tension pneumothorax. But let us be real for a moment: a checklist is only as good as the hands implementing it.
Deconstructing the primary assessment sequence: The critical phases
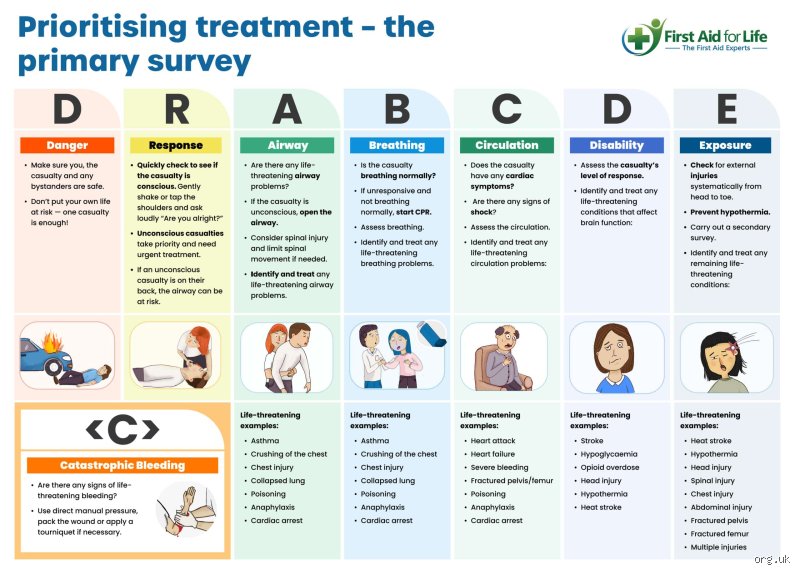
Let us break down the actual mechanics of the primary assessment, starting where the rubber meets the road. Before you even touch a patient, the absolute prerequisite is scene safety, a concept drilled into every EMT since the dawn of modern emergency services. If the environment is toxic, unstable, or actively hostile, your assessment score drops to zero because you will become the second casualty. Assuming the scene is secure, your focus shifts instantly to the letter C—or more accurately, the massive prefix.
Catastrophic hemorrhage: Stopping the clock before it runs out
If a patient is bleeding out from a femoral artery laceration, they can die in less than 60 seconds. That is why massive external bleeding now supersedes everything else. You apply a CoTCCC-approved tourniquet high and tight, or you pack the wound with hemostatic gauze immediately. People don't think about this enough: a person without blood cannot transport oxygen, rendering any subsequent airway management completely useless. I once witnessed a rookie paramedic spend two minutes attempting a difficult intubation on a victim with a severed popliteal artery; we are far from optimal care when the basics are eclipsed by complex interventions.
Airway management with simultaneous cervical spine stabilization
Once the massive bleeds are choked off, you move to the airway. Is it patent? If the patient can speak in full, coherent sentences, you have your answer, which explains why a simple hello is the fastest diagnostic tool in your arsenal. Yet, if they are unconscious, things get tricky because the tongue is the most common cause of airway obstruction in obtunded individuals. You must open the airway using a modified jaw-thrust if trauma is suspected, minimizing cervical spine movement, or a head-tilt chin-lift for medical emergencies. As a result: an open pathway allows for the next vital phase.
Breathing and ventilation: Assessing the respiratory mechanics
An open airway means nothing if the lungs cannot exchange gases. You look, listen, and feel for chest rise, respiratory rate, and effort, keeping a sharp eye out for life-threatening pathologies like a open pneumothorax or flail chest. This is where you might need to apply a chest seal or perform a needle decompression in the field. Statistically, respiratory compromise accounts for approximately 14% of preventable trauma deaths, making this phase an absolute priority before you even think about checking a peripheral pulse.
Circulation and perfusion: The internal fluid dynamics
Now we look at internal plumbing. When determining what is the correct order for primary assessment, circulation takes the fourth spot assuming massive external bleeding was controlled at the very beginning. Here, we are looking at central versus peripheral pulses, skin color, temperature, and capillary refill time to gauge the overall state of perfusion.
Evaluating hemodynamic stability and shock index
A weak, thready radial pulse indicates a systolic blood pressure that is likely hovering dangerously below 90 mmHg. You are looking for signs of hypovolemic, cardiogenic, or distributive shock. If the radial pulse is absent but the carotid is palpable, your patient is in deep trouble. Hence, this is the exact moment you establish large-bore IV access—ideally 14 or 16-gauge catheters—or prepare an intraosseous needle if veins have collapsed. Experts disagree on the exact volume of fluid resuscitation required nowadays, with the current consensus leaning heavily toward permissive hypotension to avoid popping the clot.
Comparing alternative assessment frameworks across medical specialties
While the C-ABCDE method is the undisputed king of trauma care, alternative frameworks exist depending on the specific clinical environment you find yourself navigating.
The GCS and APGAR adaptations in specialized triage
In purely pediatric cases, for instance, the assessment often leans on the Pediatric Assessment Triangle long before you deploy a hands-on primary assessment. In neonatology, the APGAR score takes precedence within the first 5 minutes of life. The core philosophy remains identical across all these variations, though: identify what is killing the patient fastest, fix it, and only then move to the next logical step.
Common mistakes and dangerous diagnostic shortcuts
Adrenaline blinds us. In the chaotic theater of an emergency, even seasoned practitioners stumble into predictable cognitive traps, flipping the structured sequence on its head. The problem is that human intuition demands we fix the loudest, most visually dramatic injury first. This fatal flaw, known as anchoring bias, kills people every year.
The fatal distraction of peripheral trauma
Imagine a compound femur fracture spurting blood across the pavement. It looks horrific. Your brain screams at you to pack that wound immediately, yet the patient is quietly suffocating from an obstructed tongue. You cannot let dramatic injuries hijack your sequence. Let's be clear: a broken leg is irrelevant if the trachea is closed. Fixating on blood while ignoring the airway is the most frequent blunder in pre-hospital care, causing catastrophic delays in basic oxygenation.
Treating what is the correct order for primary assessment as a mere checklist
You must not view this systematic protocol as a static, bureaucratic grocery list where you check a box and move on forever. It is a dynamic, continuous loop. Practitioners often check the pulse, find it adequate, and progress to neurological evaluation, never returning to re-evaluate the circulation. Except that physiology changes in seconds. A tension pneumothorax can develop mid-assessment, turning a stable respiratory status into a lethal circulatory collapse while you are busy checking pupillary reflexes. Failure to constantly re-evaluate from the top is a systemic failure of care.
Prematurely jumping into secondary diagnostics
Pulling out a blood pressure cuff or looking for a medical alert bracelet before completing the primary walkthrough is an egregious waste of time. Why measure a precise systolic number when the radial pulse is already absent? And yet, novice medics do this constantly because numbers offer a false sense of comfort in chaos. Focus entirely on the immediate threats to life before digging for historical context.
The hidden variable of primary triage: catastrophic hemorrhage
The traditional paradigm taught for decades relied heavily on the ABC method, but modern tactical medicine changed the game. Military data forced an evolution. If a patient is exsanguinating from an arterial tear, oxygenating their lungs is entirely useless because there are no red blood cells left to carry that oxygen to the brain.
The supremacy of the modern MARCH protocol
Which explains why advanced trauma life support now prioritizes massive hemorrhage above everything else. In severe trauma situations, understanding what is the correct order for primary assessment requires you to pivot to cABC or MARCH, where catastrophic bleeding takes absolute precedence over the airway. We must apply a tourniquet within 60 seconds of contact if we want to alter the mortality curve. It is a harsh reality that traditionalists struggle to accept, but the data does not lie. Are we truly saving a life if we clear an airway only to let the patient bleed out entirely onto the concrete?
Frequently Asked Questions
Does the standard protocol change when dealing with pediatric patients?
Yes, the fundamental execution changes significantly because pediatric physiology deteriorates exponentially faster than adult systems. While the sequence of your primary assessment sequence remains structurally identical, you must prioritize aggressive respiratory intervention since 80% of pediatric cardiac arrests stem directly from respiratory failure. Infants compensate for shock exceptionally well by vasoconstricting, maintaining a deceptively normal blood pressure until they suddenly crash completely. Therefore, you must evaluate capillary refill time, which should ideally be under 2 seconds, rather than relying on standard adult blood pressure metrics. A delayed capillary refill in a child is an immediate red flag for systemic hypoperfusion.
Can you skip steps if the patient is talking normally?
When a patient greets you with a clear, coherent sentence, they instantly verify a patent airway, adequate breathing, and sufficient cerebral perfusion. This initial verbal contact allows you to rapidly compress the first three steps of the initial trauma survey into a single second of observation. But the issue remains that this baseline can vanish instantly. A patient with an inhalation injury might speak clearly now, yet their airway could swell completely shut five minutes later due to progressive edema. You must still physically inspect the oral cavity and monitor their respiratory rate to ensure that initial stability is not a temporary illusion.
What is the maximum time allowed to complete this entire evaluation?
In critical trauma scenarios, you must complete the entire patient life threat evaluation within a maximum window of 60 to 90 seconds. Time is your enemy, and every tick of the clock correlates directly with tissue ischemia. Data from global trauma registries indicates that definitive interventions occurring within the golden hour dramatically improve survival rates, meaning your field evaluation must be lightning-fast. Spending five minutes on this initial phase is an absolute failure of operational efficiency. You must identify life threats, intervene immediately as they appear, and initiate transport without a single moment of unnecessary delay.
A definitive stance on emergency priority
The rigid hierarchy of life support is not an arbitrary suggestion designed by bureaucrats to complicate your field operations. It is a battle-tested evolutionary map engineered to fight human mortality in its rawest moments. If you deviate from this sequence because you think your intuition is superior to decades of collected clinical data, you are actively jeopardizing your patient. Rigid adherence to this system saves lives, period. We must abandon the dangerous arrogance of freestyle medicine and embrace the absolute discipline of the protocol. In short, memorize the sequence, respect the physiology, and execute the steps flawlessly every single time because the margin for error is absolutely zero.