Picture the chaotic environment of a Level 1 trauma center at 3:00 AM. A 45-year-old woman arrives by ambulance from JFK Airport after a flight from Tokyo, hypoxic, tachycardic, and gasping for air. Her blood pressure is cratering. You suspect a massive clot, but wheeling her down the hall to the radiology department for a computed tomography pulmonary angiography (CTPA) might actually kill her. What do you do? This is precisely where bedside ultrasound becomes the ultimate arbiter between life and death.
The Physiology Behind the Pressure: Unpacking the Right Ventricle's Breaking Point
The human heart is an asymmetric pump, a design flaw or evolutionary marvel depending on who you ask. While the thick-walled left ventricle is built to withstand high systemic pressures, the right ventricle (RV) is a thin, compliant pouch designed purely for low-pressure, high-volume workloads. It expects minimal resistance. When a massive thrombus suddenly wedges itself into the pulmonary arterial bed, the pulmonary vascular resistance skyrockets overnight. The RV finds itself pushing against a brick wall. People don't think about this enough: the RV cannot handle sudden pressure overloads.
Acute Overload versus Chronic Adaptation
Here is where it gets tricky for the treating physician. If a patient presents with right ventricular dysfunction, how do you know if they are suffering from a sudden, catastrophic acute pulmonary embolism or if they simply have long-standing, chronic pulmonary arterial hypertension from years of severe COPD or sleep apnea? The distinction dictates your next move. If you give thrombolytics (clot-busters) to a chronic pulmonary hypertension patient by mistake, you risk causing a fatal intracranial hemorrhage for absolutely no therapeutic benefit. Yet, making the right call under pressure is brutal because both conditions make the right heart look sluggish and dilated on a standard echocardiogram screen.
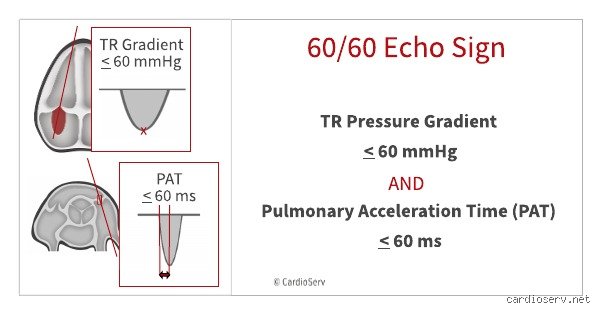
The Magic Numbers: 60 Milliseconds and 60 Millimeters of Mercury
The rule of 60 in pulmonary embolism relies heavily on spectral Doppler interrogation of the right ventricular outflow tract and the tricuspid valve. First, we look at the pulmonary acceleration time (PAat). In a healthy heart, blood gently accelerates out of the RV, peaking late in the ejection cycle. But when an acute clot obstructs the path, the pressure wave reflects back rapidly, cutting the acceleration short and forcing the peak velocity to happen in less than 60 milliseconds, often creating a visual "midsystolic notch" on the Doppler tracing. But that changes everything when you combine it with the second 60. The tricuspid regurgitant (TR) pressure gradient, calculated via the modified Bernoulli equation, must be 60 mmHg or less. Why? Because an unconditioned, acutely stressed right ventricle simply lacks the muscular hypertrophy required to generate a pressure gradient higher than 60 mmHg. If the TR gradient were 80 mmHg, that RV would have to be conditioned by months of chronic disease to pack that kind of punch.
Technical Execution at the Bedside: How to Capture the Tracings Without Losing Vital Time
Obtaining these measurements is not a task for the faint of heart or the untrained hand. It requires a meticulous approach using a phased-array ultrasound transducer placed in the parasternal short-axis view at the level of the aortic valve to visualize the right ventricular outflow tract. I have watched seasoned cardiologists struggle with this angle during a resuscitation shift at Cook County Hospital, so do not expect it to be a walk in the park. You must place the pulsed-wave Doppler sample volume just proximal to the pulmonary valve leaflets.
Once you align the cursor perfectly parallel to the blood flow, you freeze the image and measure the interval from the onset of systolic flow to its peak velocity. Is it under 60 milliseconds? If yes, you are halfway there. Next, you shift to the apical four-chamber view. Here, you apply continuous-wave Doppler across the tricuspid valve to capture the maximum velocity of the regurgitant jet, squaring that velocity and multiplying it by four. If that calculated gradient sits comfortably below the 60 mmHg ceiling, the rule of 60 in pulmonary embolism is fully satisfied. The issue remains that getting clean signals in a tachypneic patient who is hyperventilating at 40 breaths per minute is an absolute nightmare. Honestly, it's unclear why more textbooks don't emphasize how often suboptimal windows ruin this calculation.
Experts disagree on whether the rule should be utilized by novice sonographers. Some argue it should be reserved strictly for fellowship-trained echocardiographers, but when a patient is actively dying in front of you, waiting forty minutes for a cardiology consult is a luxury nobody can afford. You use the tools you have.
Clinical Specificity: Why the Rule of 60 in Pulmonary Embolism Beats General RV Dilation
Every medical student learns that a dilated right ventricle suggests a clot. Except that it doesn't always, or at least, not specifically. General signs like a dilated RV or an altered RV-to-LV ratio greater than 1.0 are notoriously sensitive but horribly non-specific; they appear in cases of acute right ventricular infarction, severe asthma exacerbations, and advanced ARDS. We need something that points directly to the pulmonary vasculature's sudden mechanical blockage. The rule of 60 in pulmonary embolism delivers exactly that kind of diagnostic precision by evaluating the actual dynamics of the blood flow rather than just the static size of the cardiac chambers.
A landmark clinical trial published in the European Heart Journal evaluated these specific Doppler parameters in patients presenting with suspected acute vascular obstruction. The researchers demonstrated that while isolated RV dilation had a specificity hovering around a dismal 50%, the presence of the rule of 60 signs pushed the diagnostic specificity past 94%. That is a massive leap forward in diagnostic certainty. As a result: when you see this specific pattern, you can be highly confident that you are looking at a fresh, mechanical obstruction within the pulmonary tree, allowing for a much safer initiation of aggressive anticoagulation or systemic reperfusion therapies right there in the resuscitation bay.
An Alternative to the Rule: Comparing the 60/60 Sign to McConnell's Sign
No discussion regarding echocardiography in acute vascular emergencies is complete without mentioning its famous cousin, McConnell's sign. Described in 1996 by Dr. W. Robert McConnell, this sign describes a distinct regional wall motion abnormality where the mid-free wall of the right ventricle is completely akinetic, yet the absolute apex of the heart retains normal, hyperkinetic contractility. It looks like the apex is bouncing or pulling the dead weight of the rest of the flatlined right ventricular wall along with it. It is highly visual, dramatic, and easily recognized even by clinicians who are relatively new to point-of-care ultrasound.
But we are far from having a perfect single test. While McConnell's sign is undeniably easier to spot during a chaotic code blue than measuring precise Doppler acceleration times, recent data suggests it is not as bulletproof as we once believed. Studies have confirmed that McConnell's sign can manifest during cases of acute right ventricular infarction, which completely muddies the clinical waters since the treatment pathways for a coronary occlusion versus a massive pulmonary clot are drastically different. Which explains why combining McConnell's sign with the quantitative rigor of the rule of 60 in pulmonary embolism provides a much sturdier diagnostic safety net than relying on visual gestalt alone. In short, use both if you can, but trust the hemodynamics when they conflict.
Pitfalls and Blunders: Where Clinicians Stumble
The Illusion of the Isolated Metric
You cannot look at a single echocardiographic variable in a vacuum. Pulmonary artery acceleration time is sensitive, but it fluctuates wildly under the influence of preexisting chronic pulmonary hypertension. Misinterpreting isolated acceleration times leads straight to diagnostic failure. If a patient presents with an acceleration time of 55 milliseconds, your reflexes might scream acute blockage. The problem is that severe, long-standing left-heart disease can mimic this exact signature without a single clot sitting in the pulmonary tree.
Overlooking the Tricuspid Gradient Cutoff
What happens when the tricuspid regurgitant jet pressure gradient hits 65 mmHg? It completely invalidates the calculation. Because acute right ventricular overload simply cannot generate such massive pressures overnight, a high gradient proves chronic remodeling. But clinicians frequently forget this rule of 60 in pulmonary embolism threshold during chaotic emergency room resuscitations. They see a shortened acceleration time, notice a high tricuspid gradient, and mistakenly attribute both to an acute event. Let's be clear: an unyielding right ventricle requires months, not minutes, to hypertrophy enough to pump against those extreme pressures.
The Misconception of Universal Applicability
Is every patient with right heart strain a candidate for this diagnostic shortcut? Absolutely not. Tachycardia above 130 beats per minute distorts the Doppler envelope. Why? Because shortened diastole truncates the very waveforms you need to measure accurately, rendering the rule of 60 in pulmonary embolism criteria utterly useless in hyperdynamic shock states.
The Hidden Nuance: Phasic Flow Dynamics
The M-Shape Notch Phenomenon
Expert echocardiographers look far beyond mere numerical thresholds to find the truth. They hunt for mid-systolic deceleration, a distinct notch in the right ventricular outflow tract flow velocity profile. This notch represents a physical reflection wave traveling back from the sudden vascular obstruction. When the forward stroke volume collides with a massive central clot, the pressure wave rebounds violently. This creates a temporary drop in velocity right in the middle of ejection. Which explains why a sharp, early notch combined with a borderline acceleration time carries far more diagnostic weight than a numbers-only checklist. It is a visual manifestation of acute physical impedance, a hemodynamic echo of a sudden mechanical disaster.
Frequently Asked Questions
How accurate is the rule of 60 in pulmonary embolism compared to McConnell's sign?
While McConnell's sign boasts a specificity hovering around 94 percent, its sensitivity remains notoriously low at roughly 77 percent in acute settings. By comparison, integrating the rule of 60 in pulmonary embolism into your assessment yields a positive predictive value exceeding 91 percent when both criteria are met simultaneously. The issue remains that relying on regional wall motion abnormalities alone can cause you to miss smaller, subsegmental clots. Diagnostic accuracy spikes dramatically because combining flow dynamics with pressure gradients filters out the chronic pulmonary hypertension mimics that frequently fool an isolated McConnell's sign evaluation.
Can this rule be safely applied to pregnant patients suspected of having a clot?
Pregnancy alters maternal hemodynamics by increasing baseline cardiac output by up to 50 percent and lowering systemic vascular resistance. Can we trust standard Doppler calculations under such hypervolemic conditions? Yes, yet you must interpret the results with extreme caution because gestational physiology naturally shortens pulmonary acceleration times even without pathology. A baseline pregnant patient might exhibit an acceleration time of 72 milliseconds, meaning the margin for diagnosing a true acute right ventricular strain narrows significantly. As a result: clinicians must rely on a tricuspid regurgitant gradient strictly below the 60 mmHg cutoff to ensure gestational volume overload isn't misdiagnosed as an acute vascular obstruction.
What should a clinician do if the two components of the rule yield conflicting data?
When an acceleration time drops to 50 milliseconds but the tricuspid regurgitant gradient measures 75 mmHg, the rule breaks down entirely. This conflict explicitly points toward chronic pulmonary vascular remodeling rather than an acute embolic event. Because an unconditioned right ventricle cannot immediately generate pressures that high, you must halt the protocol and look for alternative explanations. In short, discordant data demands immediate cross-sectional imaging via computed tomography pulmonary angiography to definitively map the pulmonary vasculature and rule out a superimposed acute clot on chronic disease.
A Definitive Stance on Right Heart Hemodynamics
Echocardiography is a dynamic window into failing physiology, not a rigid ledger of static numbers. Ultrasound operators who demand perfect mathematical harmony from a crashing patient are chasing a ghost. Prioritizing functional flow dynamics over traditional, slow diagnostic pathways saves lives when seconds dictate the clinical outcome. We must stop treating these specific bedside criteria as optional luxury metrics reserved only for cardiology fellows. The emergency manual needs an overhaul that puts right ventricular outflow tract evaluation at the forefront of resuscitation. Relying blindly on systemic blood pressure to dictate thrombolysis is an archaic practice that ignores the subtle, early warnings hidden within the pulmonary valve's Doppler envelope.