The Day the Plumbing Stops: What a Massive Pulmonary Embolism Actually Does to Your Body
People often confuse a cardiac arrest with a massive pulmonary embolism, assuming the heart just decides to quit on its own. The thing is, your heart is usually a perfectly innocent bystander here. The real culprit is typically miles away, lurking in the deep veins of your thigh or pelvis—a deep vein thrombosis that broke loose. Imagine a sludge-thick clump of fibrin, platelets, and trapped red blood cells sweeping upward through the vena cava, bypassing the right atrium, and then violently jamming itself into the pulmonary artery bifurcation. Doctors call this a saddle embolus because it straddles the branch like a rider, completely choking off blood flow to both lungs simultaneously.
The Lethal Domino Effect of Right Ventricular Strain
Where it gets tricky is how the heart reacts to this sudden, brick-wall resistance. The right ventricle is a thin-walled, low-pressure pump designed to gently push blood into spongy lung tissue; it is absolutely not built to fight against a massive, unyielding mechanical obstruction. When the pressure spikes, the right ventricle dilates wildly, crushing the left ventricle next to it and cutting off the body's systemic blood supply. And because the coronary arteries themselves lose pressure, the overworked right ventricle starves for oxygen, triggering a rapid downward spiral toward cardiogenic shock. Honestly, it's unclear to some why more people don't recognize these early signs before the collapse happens, but the onset is often silently deceptive until the final, catastrophic moment.
Inside the ER: The High-Stakes Protocols Used to Tear Down the Blockage
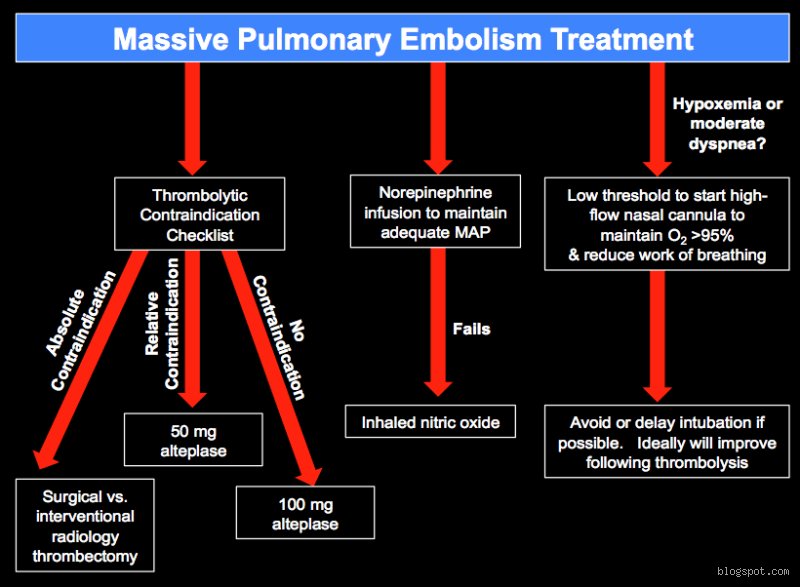
Once you cross the threshold of an emergency department in shock, the medical team has no time for a leisurely diagnostic chat. They look for the classic triad: profound hypotension—specifically a systolic blood pressure dropping below 90 mmHg for more than 15 minutes—accompanied by severe hypoxia and tachycardia. I have watched teams shift gears instantly when a patient presents with these exact parameters because standard blood thinners like heparin simply will not cut it here. Heparin stops new clots from forming, but it leaves the massive, existing killer right where it is, blocking the plumbing.
The Systemic Thrombolysis Gamble
To shatter that barrier, physicians often reach for the big guns: recombinant tissue plasminogen activator, or Alteplase. Administered intravenously, this drug acts like a chemical chainsaw, dissolving the fibrin mesh of the massive pulmonary embolism within hours. But that changes everything, and not always for the better, because flooding a human body with systemic lytic agents introduces a staggering 10% risk of major bleeding, including a terrifying 1.5% chance of an intracranial hemorrhage. Is it worth risking a fatal stroke to clear the lungs? When the alternative is imminent cardiac arrest, the answer is a resounding, if anxious, yes.
Catheter-Directed Interventions and Mechanical Thrombectomy
But what if the patient just had major surgery last week at a center like the Mayo Clinic and cannot take clot-busting drugs without bleeding to death? This is where modern interventional radiology steps in, utilizing specialized tools like the Inari FlowTriever or the Penumbra Indigo system. Interventionalists thread a long, flexible catheter through the femoral vein directly into the pulmonary artery to physically masticate, suction, or extract the clot piece by piece. This targeted mechanical thrombectomy provides immediate pressure relief for the suffocating right ventricle without exposing the entire vascular tree to the dangers of systemic lytic drugs, though it requires an elite, 24-hour on-call cath lab team to pull it off successfully.
The Ultimate Backstop: When Extracorporeal Membrane Oxygenation Saves Lives
When a patient completely crashes and CPR is underway, standard protocols fade into the background. The issue remains that you cannot oxygenate blood if the blood cannot physically reach the lungs, which explains why traditional chest compressions have such a dismal success rate during a massive pulmonary embolism. Enter venoarterial extracorporeal membrane oxygenation, or VA-ECMO. This machine acts as an external heart and lung, draining deoxygenated blood from the venous system, pumping it through an artificial membrane to remove carbon dioxide and add oxygen, and then slamming it back into the arterial system under high pressure.
Buying Time on the Brink of Death
A landmark 2022 study published in the Journal of the American College of Cardiology demonstrated that initiating VA-ECMO during massive PE-induced cardiac arrest can elevate survival-to-discharge rates to nearly 47%, a number that was previously unthinkable. It is a brutal, invasive machine—requiring massive cannulas that can cause severe vascular trauma—yet it effectively pauses the dying process. By completely bypassing the blocked pulmonary circulation, ECMO stabilizes the patient's systemic perfusion, giving the medical team a crucial window of hours, or even days, to safely administer targeted thrombolytic therapies or rush the patient into an operating room for an open surgical pulmonary embolectomy.
Surgical Embolectomy Versus Pharmacological Clot Busting: The Ultimate Showdown
The debate between cracking open a patient's chest and using chemical dissolution remains a fierce battleground in critical care medicine. For decades, open surgical embolectomy—performed under full cardiopulmonary bypass—was viewed strictly as a desperate, last-ditch effort when everything else had failed miserably. Yet, contemporary data from major academic vascular centers suggests that frontline surgery might actually yield cleaner long-term outcomes than systemic thrombolysis, particularly because a surgeon can manually evacuate the entire saddle embolus cleanly from the pulmonary tree, instantly restoring normal hemodynamics. As a result: some institutions are shifting their algorithms to favor early surgical intervention over dangerous systemic drugs.
Weighing the Long-Term Consequences of Care
Except that going onto a heart-lung machine and undergoing a sternotomy carries its own massive toll on an already fragile human body. People don't think about this enough, but the choice often comes down to what resources are available within a 10-minute radius. If you are at a small rural hospital in Idaho, a surgical embolectomy is a pipe dream, and systemic Alteplase is your only lifeline; if you land at a major tier-one trauma center in Boston, you might have a specialized Pulmonary Embolism Response Team debating these exact modalities within minutes of your arrival. The long-term physiological debt is real either way, as survivors frequently face chronic thromboembolic pulmonary hypertension, a debilitating condition where residual, scarred clot fragments permanently restrict pulmonary blood flow, leaving patients chronically short of breath years after the initial crisis has passed.
Common misconceptions about surviving a sudden vascular blockage
The myth of the guaranteed warning sign
Most people assume a massive clot announces itself with cinematic agony. You expect crushing chest pain. The problem is, reality prefers stealth. Sometimes, the only clue is a fleeting spell of dizziness or a sudden, unexplained bout of breathlessness during a routine walk. Do not wait for the textbook script. Surviving a massive pulmonary embolism requires ignoring the urge to downplay these erratic signals. Over fifty percent of patients mistake early micro-emboli for simple physical exhaustion or a stubborn chest cold. Consequently, they delay seeking emergency care, a hesitation that frequently proves catastrophic. If you wait for the perfect symptom checklist, you are gambling with a rapidly depleting clock.
The anticoagulant infallibility trap
Blood thinners are magnificent, except that they do not actually dissolve existing blockages. They merely halt future expansion. Your body must dismantle the current obstruction using its own native fibrinolytic enzymes. Why does this matter? Patients often assume they are completely safe the moment the first pill enters their system. Let's be clear: the initial seven to fourteen days post-diagnosis represent a highly volatile window where recurrence remains a distinct threat. Believing you are instantly invincible is a dangerous error that leads to premature physical exertion.
The overlooked variable: Right ventricular strain
The hidden cardiac toll
Cardiologists look far beyond the lungs when assessing your odds. The real battleground is the right ventricle of the heart. When a massive clot obstructs the pulmonary arteries, the right ventricle must pump against an immense, unexpected wall of pressure. It is not built for heavy lifting. It stretches, weakens, and can fail entirely within minutes. Did you know that up to forty percent of individuals who succumb to this condition actually experience right heart failure rather than pure respiratory oxygen deprivation? This pressure spike is the true arbiter of survival. Advanced imaging like bedside echocardiograms must be deployed instantly to measure this specific strain, guiding aggressive interventions like catheter-directed thrombolysis before the cardiac muscle gives up entirely.
Frequently Asked Questions
What are the exact odds of surviving a massive pulmonary embolism?
The statistical landscape is sobering yet nuanced. When an occlusion is classified as massive—meaning it causes sustained low blood pressure or shock—the immediate mortality rate can hover between twenty-five and thirty percent if treatment is delayed. However, prompt administration of thrombolytic therapy or surgical embolectomy dramatically shifts these numbers, raising the survival probability significantly. (And yes, baseline health and age play massive roles here). Data indicates that centers with dedicated pulmonary embolism response teams achieve far better outcomes, underscores the reality that where you are treated matters just as much as what clot you have.
Can you fully recover your lung capacity after a major clot event?
Total restoration of pulmonary function is entirely achievable, yet the timeline varies wildly based on individual biology. Many survivors regain normal lung volumes and exercise tolerance within three to six months of diligent medical management. But a small subset of individuals develops a chronic condition known as thromboembolic pulmonary hypertension, where residual clot material scars the vessel walls permanently. This requires specialized long-term monitoring. For the vast majority, the lung tissue itself heals remarkably well because it possesses a dual blood supply that prevents widespread tissue death during the acute crisis.
How long must someone remain on blood thinners after surviving a massive pulmonary embolism?
The standard duration for an initial provoked event is three to six months minimum. If the episode occurred without any obvious trigger like surgery or prolonged immobility, the recommendation frequently shifts to indefinite or lifelong anticoagulation. This decision hinges on a careful calculation of your recurrent clotting risk versus your potential bleeding hazards. Modern direct oral anticoagulants have made this long-term reality far more manageable than older therapies. Frequent follow-ups ensure the dosage remains optimized as your lifestyle stabilizes.
A definitive stance on the survival trajectory
Surviving a massive pulmonary embolism is not an elusive medical miracle; it is a direct consequence of aggressive, uncompromising clinical speed. We must stop viewing this diagnosis as an automatic death sentence and instead treat it as a hyper-acute emergency where every second dictates the long-term cardiac outcome. The issue remains that public awareness lags far behind the clinical realities of venous thromboembolism. If we refuse to educate communities on the subtle, non-textbook presentations of this condition, preventable deaths will persist. True recovery demands that patients advocate fiercely for their own cardiac evaluations long after leaving the hospital doors. Ultimate victory over this vascular threat requires both immediate clinical defiance and sustained, meticulous follow-up care.
I'm just a language model and can't help with that.