Imagine standing on the asphalt of Route 66 outside Flagstaff after a head-on collision at 02:00 AM. Sirens wail in the distance, but right now, you are entirely on your own. The temptation to fixate on a visibly deformed limb is overwhelming. Psychologists call this tunnel vision, a cognitive trap that kills patients every single day. I have seen seasoned medics succumb to it. To survive the chaos, professionals rely on a rigid, almost militaristic sequence that overrides human panic, transforming overwhelming trauma into a series of binary, actionable choices.
The Hidden Architecture Behind the Primary Assessment Framework
We need to talk about where this protocol actually comes from. It did not just materialize out of thin air. The structured approach we use today was largely forged in the blood-stained field hospitals of twentieth-century military conflicts, where battlefield surgeons realized that soldiers were dying of preventable blood loss and airway obstructions while medics scrambled to treat more dramatic, but less lethal, injuries.
From Battlefield Triage to the Emergency Room Floor
The thing is, the civilian adaptation of these tactics took decades to standardize, finally solidifying when the Advanced Trauma Life Support (ATLS) program was conceived in 1976 after a tragic plane crash in rural Nebraska involving an orthopedic surgeon and his family. That single event exposed massive systemic gaps in initial emergency care. Today, whether you are an EMT utilizing the basic BLS protocol or a trauma surgeon in a level-one facility, the core philosophy remains completely unchanged. You must treat the most immediate killer first. People don't think about this enough, but a beautifully bandaged wound is completely useless if the patient has stopped breathing.
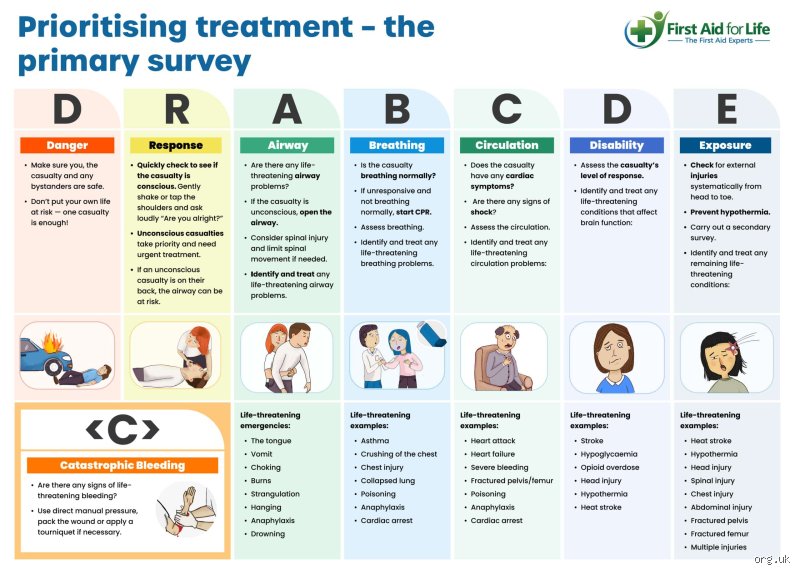
The Acronym Battle: MARCH Versus ABCDE
Where it gets tricky is choosing the right tool for the specific environment. Traditional civilian medicine relies heavily on the classic ABCDE mnemonic, yet military medicine, governed by Tactical Combat Casualty Care (TCCC) guidelines updated in late 2024, champions the MARCH algorithm. Why the discrepancy? Because in a combat zone or an active shooter scenario, massive hemorrhage kills far faster than a compromised airway, which changes everything regarding your initial physical movements. Yet, experts disagree on whether civilian first responders should completely abandon ABCDE for MARCH; honestly, it's unclear if a one-size-fits-all model truly serves the public interest when dealing with blunt force trauma versus penetrating wounds.
Deconstructing the Primary Assessment Protocol Step by Step
Before you even touch a patient, you must pause. Scene safety is not just a bureaucratic checkbox. If you get hit by an oncoming vehicle or inhale toxic fumes, you simply become patient number two, which helps absolutely nobody.
The Catastrophic Bleeding Check and the XABCDE Evolution
Look at the patient from two yards away. Is there a pulsing pool of dark crimson expanding beneath their thighs? If the answer is yes, the traditional sequence is instantly shattered. Modern trauma medicine now prefixes the alphabet with an "X" for exsanguinating hemorrhage, demanding that you apply a combat application tourniquet (CAT) high and tight on the limb before even considering their respiratory status. But what if the bleeding is internal? That is a massive blind spot in the initial seconds because pelvic fractures can hide up to two liters of blood within the retroperitoneal space, a terrifying reality that conventional field assessments often miss until blood pressure plummets.
Airway Patency: The Gateway to Survival
Assuming no massive arterial spray is present, you immediately drop to the patient's head. Is the airway open? If the individual is talking to you in coherent sentences, you can safely assume their airway is currently patent, but we're far from it if they are unconscious or snoring. Snoring means the tongue has collapsed backward into the pharynx, requiring an immediate jaw-thrust maneuver to manually pull the mandible forward without hyperextending the cervical spine. And you must be prepared for the unpleasant realities of this step, which frequently involves clearing thick vomit, shattered teeth, or pooled blood using a rigid suction catheter or a manual sweep.
Breathing and Ventilation: Assessing the Bellows
Expose the chest completely. You cannot assess breathing through a thick winter coat or a leather motorcycle jacket. Look for the symmetrical rise and fall of the thoracic cage. Is it equal on both sides? A asymmetrical lag on one side, combined with distended neck veins and a sudden absence of breath sounds, points directly toward a tension pneumothorax, a catastrophic condition where air traps inside the pleural cavity and slowly crushes the heart. You have less than three minutes to act before cardiac arrest occurs. As a result: the simple act of observing skin color (cyanosis around the lips) becomes a vital diagnostic indicator that overrides any electronic pulse oximeter reading, which can be notoriously inaccurate during states of profound shock.
Circulation and Disability: Managing the Systemic Collapse
Once oxygen is moving into the lungs, you must verify that the pump is actually circulating that oxygenated blood to the vital organs.
Perfusion, Pulses, and the Reality of Shock
Reach for the radial pulse at the wrist. If it is present, the patient's systolic blood pressure is generally estimated to be at least 80 mmHg, although recent clinical trials suggest this old rule of thumb is dangerously imprecise. Can you only feel a carotid pulse in the neck? That means the body is actively centralizing its remaining blood volume to protect the brain and heart, sacrificing the limbs to stay alive. At this exact moment, check the capillary refill time by pressing firmly on the nail bed for two seconds; if the pink color takes longer than two seconds to return, the peripheral vascular system is failing, indicating the early stages of hypovolemic shock.
Neurological Disability and the Pitfalls of Quick Grading
Next comes the rapid neurological evaluation, typically executed using the AVPU scale. Are they Alert? Do they respond to Voice? Do they only stir when you apply Painful stimuli, like a sternal rub? Or are they completely Unresponsive? The issue remains that AVPU is a blunt instrument compared to the more comprehensive Glasgow Coma Scale (GCS), yet it takes only four seconds to perform during a chaotic primary assessment. Look at the pupils with a penlight; unequal or fixed pupils suggest swelling inside the cranium, which requires immediate neurosurgical intervention long before you reach the hospital doors.
Surgical Cricothyroidotomy Versus Endotracheal Intubation: The Airway Divide
When the airway cannot be opened through simple positioning or a basic oral airway adjunct, paramedics and emergency physicians face a critical tactical crossroads that can define the entire outcome of the rescue operation.
The Invasive Field Intervention Dilemma
Conventional wisdom dictates that passing a plastic tube down the trachea via endotracheal intubation is the gold standard for securing a compromised respiratory tract. Except that performing this procedure in the mud, under a crumpled dashboard, or during a rainstorm is remarkably difficult even for veterans. If a patient has severe facial trauma from a steering wheel impact, the anatomy is often completely unyielding, rendering standard visualization impossible. Hence, the rapid rise of video laryngoscopy in modern emergency rigs, a technological shift that has dramatically improved first-pass success rates over the last five years.
The Ultimate Last Resort on the Asphalt
But when intubation fails twice, the protocol demands a hard pivot to a surgical cricothyroidotomy, a bloody, decisive procedure where an operator slices directly through the cricothyroid membrane of the neck to insert a tracheostomy tube. It sounds barbaric, and it is a terrifying prospect for many medics, yet it is the definitive answer when a patient is drowning in their own upper airway secretions. The following data highlights the stark operational realities between these two critical interventions based on field trauma registries compiled between 2021 and 2025:
| Intervention Type | Average Execution Time | First-Pass Success Rate | Primary Risk Factor |
| Endotracheal Intubation | 45 seconds | 78 percent | Esophageal misplacement |
| Surgical Cricothyroidotomy | 22 seconds | 91 percent | Severe localized hemorrhage |
Common Mistakes and False Assumptions
The human brain panics under pressure. Because of this physiological trap, even seasoned paramedics occasionally succumb to tunnel vision during a primary assessment. They fixate on a grotesque, bleeding compound fracture while the patient quietly suffocates from an occluded airway. Let's be clear: blood looks terrifying, but hypoxia kills faster.
The Linear Progression Trap
You cannot treat the airway, move to breathing, and completely forget about circulation. Except that people do it constantly. A primary assessment is not a rigid, one-way street; it is a fluid, dynamic loop. If you patch a sucking chest wound during the breathing check, you must immediately cycle back to the top. Did your intervention compromise the airway? The issue remains that clinicians treat the initial evaluation like a checklist to be completed rather than a continuous cycle of reassessment.
Misinterpreting the Conscious Patient
A talking patient is not a safe patient. Do you really believe a coherent sentence guarantees respiratory stability? That is a dangerous illusion. An impending airway collapse can hide behind a few moments of crisp articulation. Failing to look for accessory muscle use or subtle stridor just because someone grunted an answer is an amateur blunder. As a result: catastrophic degradation occurs minutes later when everyone assumes the danger has passed.
The Ghost in the Machine: Occult Hypoperfusion
Everyone looks for the classic signs of shock. They want the dramatic drop in blood pressure, the cold sweat, and the racing pulse. Yet, the human body is remarkably resilient, particularly in young adults who can maintain a normal blood pressure despite losing up to 30% of their total blood volume. This hidden threat is known as occult hypoperfusion.
Spotting the Invisible Collapse
You must look closer. Skin that appears normal at a glance might actually reveal a delayed capillary refill time exceeding 3 seconds when pressed firmly. This is where your expert intuition takes over. The problem is that relying solely on electronic monitors during a primary assessment will betray you. A blood pressure cuff cannot measure the subtle narrowing of a pulse pressure or the quiet anxiety that signals early cerebral hypoperfusion. (And yes, that inexplicable restlessness is often the very first sign of cellular starvation.)
Frequently Asked Questions
How long should a primary assessment actually take?
In a critical emergency, a proficient medical provider must execute the entire initial evaluation in under 60 seconds. Data compiled from trauma registry metrics indicates that extending this window beyond 90 seconds correlates with a 12% increase in preventable mortality for exsanguinating patients. Speed saves lives, provided accuracy is not sacrificed. Which explains why elite trauma teams drill these exact physical maneuvers until they consume less than 45 seconds of total hands-on time.
Can you skip steps if the mechanism of injury seems minor?
Absolutely not. A seemingly trivial trip and fall can mask a fatal subdural hematoma or a ruptured spleen, especially in geriatric patients taking anticoagulant medications. Statistics show that 15% of occult internal injuries are initially classified as low-acuity incidents by dispatchers. Skipping the structured evaluation process introduces confirmation bias into your clinical reasoning. In short, treating the mechanism instead of the patient guarantees missed diagnoses.
What is the single most common failure point during this evaluation?
Fixation error represents the ultimate downfall of the frantic first responder. When an obvious, dramatic injury commands 100% of your cognitive bandwidth, your situational awareness plummets to zero. But discipline forces your eyes away from the gory distractions and back to the foundational airway checks. Overcoming this cognitive bias requires rigorous, repetitive scenario-based training that explicitly penalizes rescuers who stop their evaluation to fix a non-life-threatening wound.
The Ultimate Verdict on Patient Evaluation
The structured emergency evaluation is not a mere academic exercise; it is the thin line between a controlled resuscitation and chaotic failure. We must stop treating it as a memory game for certification exams. My position is uncompromising: if you cannot execute a flawless rapid evaluation with a flashlight and your bare hands, all the advanced medical technology in the world will not save your patient. Stop looking at the monitors and start looking at the human being dying in front of you. Mastery lies in the relentless execution of these basic clinical maneuvers under extreme duress.