The Post-Prostatectomy Anatomy: Where It Gets Tricky for Erectile Function
Most men view the prostate purely through the lens of cancer screenings or reproductive health, ignoring its proximity to the mechanism that controls erections. When a surgeon performs a radical prostatectomy—whether to treat localized prostate cancer or severe benign conditions—they do not just remove a walnut-sized gland. They operate in a hyper-dense anatomical crossroad. The prostate is literally wrapped in a fragile network of microscopic blood vessels and nerves called the neurovascular bundles. These microscopic fibers are the electrical wiring for your penis. If the current cannot flow from the brain down to the erectile tissues, nothing happens.
The Myth of the Independent Erection
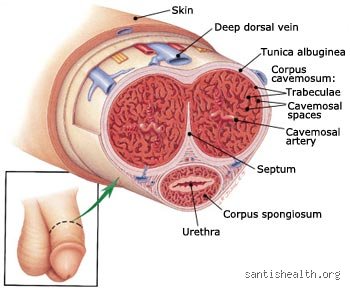
People don't think about this enough: your prostate does not create erections, but its removal can easily destroy them. I have seen countless patients leave the hospital assuming that because their penis looks the same, it should function the same. It is a devastating misconception. The corpora cavernosa—the two spongy chambers inside the penis—rely on a precise chemical cascade triggered by those pelvic nerves. When the nerves are traumatized, the cascade stops dead. Yet, the prostate itself is responsible for producing about 30% of seminal fluid. Consequently, even if you achieve an erection later, you will experience what medicine calls a dry orgasm. The sensation remains, but the physical payload is gone forever. This is where conventional wisdom falters; many assume a dry orgasm means a lesser orgasm, which is simply psychologically untrue for most men who adapt over time.
Nerve-Sparing Surgery vs. Non-Nerve-Sparing Reality
During a procedure at a specialized center like the Johns Hopkins Brady Urological Institute, surgeons attempt what is called a nerve-sparing prostatectomy. It sounds elegant. In practice, it is a game of millimeters. If the cancer has breached the prostatic capsule, the surgeon must prioritize saving your life over saving your sex life, meaning those vital nerves are intentionally sacrificed. But even in a perfect bilateral nerve-sparing surgery, those nerves are stretched, bruised, and deprived of blood during the operation. They fall into a state of deep shock called neuropraxia. Think of it as a severe concussion of the pelvic nerve network. Recovery does not take days; it takes months, sometimes up to 24 months, for these microscopic pathways to regenerate and fire properly again.
The Pharmacology of Sildenafil: How Viagra Interacts with a Mutated Anatomy
To understand why Viagra might fail after surgery, we have to look at how sildenafil works on a molecular level. It is not an aphrodisiac. It will not cause an erection spontaneously just because it is circulating in your bloodstream. Viagra is a PDE5 inhibitor. It works by blocking the phosphodiesterase type 5 enzyme, which normally breaks down a molecule called cyclic guanosine monophosphate (cGMP). More cGMP means the smooth muscles in the penile arteries relax, allowing blood to rush in. Except that there is a massive catch. To get that initial burst of cGMP, your body needs nitric oxide. And guess where that nitric oxide comes from? It is released by the very cavernous nerves that were just disturbed during your surgery.
[Image of mechanism of action of PDE5 inhibitors]The Nitric Oxide Dilemma
This is precisely where the pharmaceutical math breaks down for many men post-surgery. If your nerves are severed or severely damaged, they cannot release nitric oxide. Without nitric oxide, there is no cGMP production. If there is no cGMP production, Viagra has absolutely nothing to protect or amplify. It is like stepping on the gas pedal of a car that has no engine. The plumbing is perfectly capable of holding blood, but the electrical signal to open the floodgates never arrives. Because of this, clinical efficacy trials show that while Viagra has an 80% success rate in the general population, that number plummets drastically in the immediate months following a prostatectomy. You can take the maximum dose of 100mg, and the result will be total silence if the nerve pathways are offline.
The Problem of Penile Hypoxia
The issue remains that a non-functioning penis is a dying tissue environment. When you do not have nocturnal erections—which normally happen three to five times a night during REM sleep to oxygenate the tissue—the penile structures starve. This lack of oxygen, or penile hypoxia, leads to irreversible structural changes. Within just a few months of inactivity, the smooth muscle cells inside the corpora cavernosa begin to transform into rigid, non-elastic collagen fiber. As a result: the penis loses its ability to expand, leading to measurable shortening and permanent venous leakage. This is why waiting around for natural recovery is a terrible strategy. Even if your nerves eventually wake up two years later, the physical tissue may have scarred so badly that it can no longer trap blood.
The Timeline of Recovery: Why Timing Altering the Outcome Changes Everything
When does Viagra work if you have no prostate? Honestly, it is unclear in the first twelve weeks. Early on, the clinical failure rate is discouragingly high. A landmark study published in The Journal of Urology tracked men using sildenafil post-prostatectomy and found that response rates evolve dramatically over time. During the first 3 months, almost nobody responds to oral medications because the nerves are in that state of profound hibernation. But patience is required here. By month 12 to 18, as the nerves slowly heal, men who previously saw zero results from Viagra suddenly start experiencing partial erections. It is a slow, agonizingly gradual awakening that requires persistence.
The Concept of Penile Rehabilitation
This long timeline gave rise to a medical strategy known as penile rehabilitation, pioneered by institutions like Memorial Sloan Kettering Cancer Center in New York. The philosophy contradicts conventional wisdom: you do not take Viagra to have sex; you take it as physical therapy for your penis. Urologists frequently prescribe a low daily dose of a PDE5 inhibitor—often Cialis (tadalafil) 5mg, or Viagra 25mg three times a week—starting just weeks after the urinary catheter is removed. The goal is not penetration. The goal is to force a trickle of oxygenated blood into the tissues to prevent that dreaded collagen scarring. We are far from a guarantee here, as some large-scale clinical trials have questioned whether daily dosing outperforms on-demand use, but the physiological logic of keeping the tissue alive is sound.
Comparing Viagra to the Alternatives When Nerves Are Compromised
If Viagra fails because the nerve damage is too severe, you cannot just double the dose and hope for the best. That only increases side effects like headaches, facial flushing, and visual disturbances. You have to bypass the nerves entirely. Fortunately, the erectile tissue itself is usually perfectly healthy; it just needs a different chemical trigger. This is where we pivot from oral pills to local therapies that deliver vasodilators directly to the target tissue without needing an electrical signal from the pelvis.
Intracavernous Injection Therapy (ICI)
The gold standard alternative when Viagra fails is penile injection therapy, using drugs like Trimix—a customized compounding mixture of alprostadil, papaverine, and phentolamine. You use a tiny, diabetic-style needle to inject the fluid directly into the side of the penis. It sounds terrifying. Yet, the vast majority of men report that the pain is minimal, and the results are unmatched. Because these medications act directly on the smooth muscle receptors, they completely bypass the damaged cavernous nerves. Within 5 to 15 minutes, you get a rigid erection that lasts regardless of psychological stimulation or nerve integrity. In fact, Trimix boasts a success rate exceeding 90% in post-prostatectomy patients, making it the most reliable tool for early penile rehabilitation while waiting for nerve recovery.