The Anatomy of a Leak: What Exactly Are We Dealing With Here?
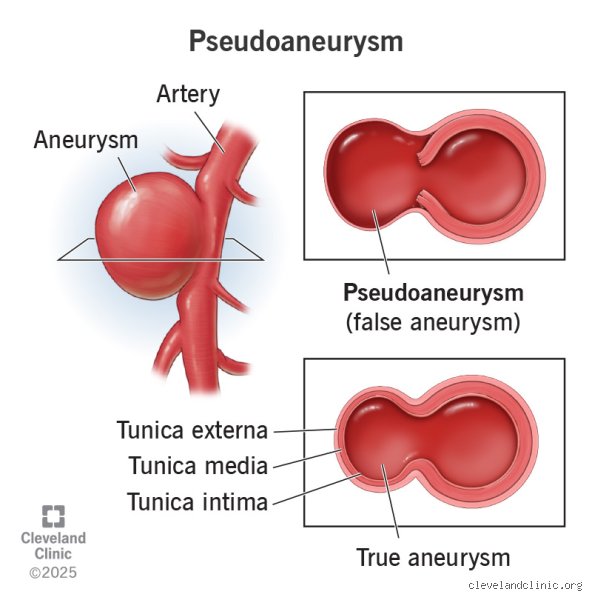
To understand the pain, we have to look at the structural deception happening beneath the skin. A true aneurysm involves all three layers of the arterial wall stretching out like an overinflated balloon. A pseudoaneurysm is an entirely different beast; it is a literal hole in the artery. Blood escapes through a breach in the tunica intima and media, but it gets contained by the outermost adventitia or, more frequently, a makeshift capsule of surrounding soft tissue and clotted hematoma. I have looked at dozens of these imaging scans, and it always strikes me how violent the process actually is.
The False Wall Illusion
The thing is, this contained puddle of blood never stops swirling. Because it maintains a direct connection to the main arterial pipeline through a narrow neck, every single heartbeat pumps high-pressure blood directly into this fragile, artificial pocket. Doctors refer to this distinct turbulent flow as the ying-yang sign when visualizing it under color Doppler ultrasound. The surrounding tissue becomes a reluctant dam holding back a river.
Why True and False Aneurysms Part Ways on the Pain Scale
People don't think about this enough: a gradual stretch hurts far less than a sudden, forced intrusion. True aneurysms can remain asymptomatic until they reach terrifying proportions, whereas a pseudoaneurysm behaves more like an expanding localized explosion. The pressure within the hematoma builds rapidly, stretching nerve endings in the vicinity until they fire off frantic distress signals to the brain. That changes everything when it comes to early diagnosis.
The Neurology of the Ache: Tracking the Pain Pathways
Where it gets tricky is mapping out exactly why one patient screams in agony while another merely complains of a vague, annoying heaviness. The primary culprit behind the severe discomfort is nerve compression. When an iatrogenic injury—say, a slip during a routine femoral artery catheterization at a clinic in Chicago—creates a false lumen, the resulting blood collection has nowhere to go except into spaces already occupied by major nerve pathways.
The Femoral Nerve Under Siege
Take the groin area, the absolute capital city of pseudoaneurysm formation due to the sheer volume of interventional cardiology procedures performed globally. If a femoral pseudoaneurysm expands by even a few millimeters, it can pin the adjacent femoral nerve directly against the tough, unyielding inguinal ligament. The result? A searing, burning pain that shoots down the anterior thigh, sometimes accompanied by a sudden, terrifying weakness in the quadriceps muscle. Is it just a localized bruise, or is the tissue quite literally suffocating? It is a question emergency room physicians must answer with Doppler probes, not guesswork.
Ischemia and the Cry for Oxygen
But the pain mechanism is actually twofold. Beyond the direct mechanical pinching of nerve fibers, the swelling mass can compress nearby smaller capillaries, completely cutting off the localized blood supply to adjacent muscles. This induces micro-ischemia. When muscle tissue is starved of oxygenated blood—even in a tiny, localized zone—it releases a torrent of lactic acid and inflammatory cytokines. This chemical cocktail irritates local nociceptors, creating that deep, sickening, unremitting ache that refuses to back down even when you change positions.
Clinical Realities: When the Throbbing Mass Signals Immediate Danger
Let us look at the hard data collected over years of vascular audits. In a landmark 2021 retrospective study analyzing vascular complications across 1,450 patients who underwent percutaneous coronary interventions, researchers found that localized pain was the primary presenting symptom in 78 percent of confirmed pseudoaneurysm cases. Yet, the remaining percentage felt almost nothing, which brings us to a frustrating medical paradox: the absence of pain does not mean you are safe.
The Silent Expanders
Why do some people walk around with a ticking time bomb without realizing it? Honestly, it's unclear, though experts disagree on whether nerve density variations or patient pain tolerance plays the bigger role. If a pseudoaneurysm forms in a deep, spacious anatomical compartment—like the profound spaces of the thigh or deep within the gluteal muscles after a traumatic injury—it can expand significantly before hitting a hard boundary. The tissue simply yields. It accommodates the growing pool of blood, delaying the onset of that crucial pressure-induced pain until the structural integrity of the entire region is compromised.
The Tell-Tale Pulsatile Mass
Except that you can often feel it even if it does not hurt yet. A classic pseudoaneurysm presents as a palpable, pulsatile mass. When you place your fingers over the swelling, it does not just sit there; it throbs in perfect, rhythmic synchronization with your pulse. Vascular surgeons will often use a stethoscope to listen for a systolic bruit—a distinct, rushing or whooshing sound caused by the blood whipping through the narrow neck into the false sac. If you hear that sound, we're far from a simple hematoma; you are listening to a structural failure in real-time.
Diagnostic Confounders: Distinguishing the False from the True
When a patient arrives at a vascular clinic complaining of post-procedural pain, sorting out the true pathology requires swift, decisive imaging. The issue remains that a simple hematoma—a standard, non-pulsatile bruise where blood has leaked and clotted without a continuous arterial connection—can look and feel remarkably similar during the first twenty-four hours. Both cause swelling, both cause localized tenderness, and both can make walking an absolute nightmare.
The Ultrasound Decider
This is where duplex ultrasonography earns its status as the gold standard of initial assessment, boasting a diagnostic sensitivity of roughly 94 percent and a specificity hovering around 97 percent. The technician glides the transducer over the painful groin or wrist, mapping the velocity of the moving cells. If they see blood rushing backward and forward through a disrupted arterial wall—the classic to-and-fro waveform—the diagnosis is locked in. As a result: the patient avoids an unnecessary exploratory surgery, and the team can plan a targeted intervention.
When the Location Changes the Stakes
We must also look at alternative sites because the groin does not hold a monopoly on this condition. With the global rise of radial artery access for cardiac catheterizations since the mid-2010s, radial pseudoaneurysms have become a distinct clinical headache. The wrist is a tight, unforgiving space; there is no loose fat to absorb an expanding hematoma. Consequently, a radial leak hurts almost instantly, compressing the median or superficial radial nerve and causing tingling in the thumb and index finger long before the actual swelling becomes visually alarming. It is a dramatic contrast to the deep, silent expansion possible in the pelvic cavity.
Common mistakes and dangerous misconceptions
The "No Pain, No Problem" fallacy
Many individuals assume that the absence of physical distress equals safety. It does not. A silent vascular disruption can masquerade as a harmless, indolent swelling for weeks before disaster strikes. Let's be clear: relying on discomfort as your primary warning system is a catastrophic medical gamble. While a true arterial wall rupture typically announces itself with agonizing force, an expanding false aneurysm can develop with zero initial sensory feedback. This happens because the surrounding tissue slowly stretches to accommodate the growing hematoma, delaying nerve compression. If you discover a pulsatile mass after a cardiac catheterization, do not wait for agony to strike before calling your physician.Confusing them with true aneurysms
Patients, and occasionally distracted clinicians, frequently conflate these two entirely distinct vascular pathologies. A true aneurysm involves the dilation of all three layers of the arterial wall. Conversely, a pseudoaneurysm is actually a contained hematoma outside the vessel, fed by a persistent hole in the arterial lumen. Why does this structural difference matter so much? The answer lies in their unpredictable stability. True aneurysms often expand over years, yet a false aneurysm can destabilize over mere hours due to fluctuating blood pressure. Treating them with a identical watch-and-wait philosophy is an oversight that frequently leads to emergent surgical intervention.Ignoring the history of recent trauma
Another frequent mistake is evaluating localized pain without reviewing recent medical charts. Did you undergo an orthopedic procedure or an arterial line placement last month? The connection between iatrogenic injury and subsequent localized throbbing is often overlooked by patients seeking routine care for what they assume is a simple muscle strain. Because the discomfort can mimic deep vein thrombosis or a localized hematoma, the actual vascular leak remains hidden.The hidden threat of late-onset nerve compression
The creeping shadow of ischemic neuropathy
Beyond the immediate structural danger, an overlooked aspect of this condition is the delayed neurological fallout. As blood pumps into the extraluminal space, the resulting tension creates a high-pressure compartment. This localized pressure gradient eventually suffocates adjacent peripheral nerves by cutting off their microscopic blood supply, known as the vasa nervorum.Why early detection saves functional mobility
What begins as a vague, dull ache can rapidly transform into permanent motor deficit or complex regional pain syndrome if the pressure is left unchecked. Except that this progression is rarely linear; it often accelerates suddenly when the hematoma breaches a new tissue plane.Diagnostic Tip: Clinicians should always perform a thorough distal neurovascular exam, checking for diminished pulses or sensory loss, whenever a post-procedural vascular complication is suspected.Medical literature indicates that up to 12% of femoral pseudoaneurysms trigger some degree of femoral nerve compression. This leads to quadriceps weakness and sensory loss along the anterior thigh. The issue remains that once a nerve undergoes prolonged ischemic starvation, the path to neurological recovery becomes exceptionally grueling, which explains why waiting for classic symptoms is so dangerous.