An Anatomy of Inconvenience: What Exactly Is This Gland Doing Down There?
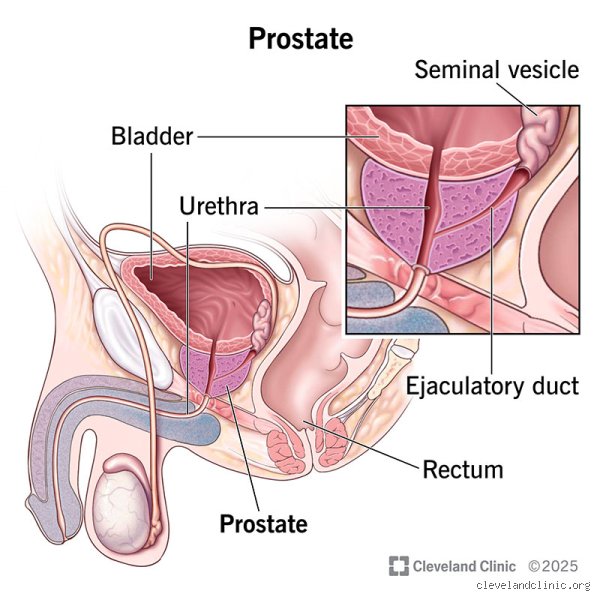
Most guys do not give this tiny piece of flesh a single thought until they find themselves staring at the bathroom wall at three o'clock in the morning, waiting for a stream that refuses to start. Let us be honest, the design is a bit of an engineering disaster. The prostate sits snugly just below the bladder, wrapped completely around the urethra like a tight donut. Why nature decided to route the main drainage pipe of the male urinary tract directly through a gland prone to swelling is anyone's guess. When you are twenty, it is the size of a walnut and behaves itself perfectly. But fast forward a few decades, and things change. The cellular machinery inside begins a slow, relentless expansion that urologists call Benign Prostatic Hyperplasia, a condition affecting roughly fifty percent of men by age fifty.
The Cellular Geography
Where it gets tricky is how the gland is partitioned into distinct zones. You have the peripheral zone, which sits toward the back and is where roughly seventy percent of prostate cancers originate. Then there is the transition zone, which wraps around the urethra and is the primary culprit behind those agonizingly frequent bathroom trips. Because these zones behave like completely different organs under the microscope, a man can have a massive prostate that makes peeing a nightmare but remains entirely cancer-free. Conversely, a tiny, normal-feeling gland can harbor a aggressive tumor. It is a biological paradox that keeps oncologists awake at night.
The True Biomechanical Purpose: Fertility, Chemistry, and Survival
So, what does it actually do when it is not causing trouble? The prostate is essentially a highly specialized chemical factory. During ejaculation, it pumps a alkaline fluid into the urethra, which makes up about thirty percent of the total semen volume. This is not just filler material. The vaginal environment is naturally highly acidic—a brilliant evolutionary defense mechanism against bacteria—but that same acid is completely lethal to incoming sperm. Without the prostate’s milky, zinc-rich secretion to neutralize that hostile environment, natural human reproduction would pretty much grind to a screeching halt.
The Role of Prostate-Specific Antigen
But the real magic trick is an enzyme called Prostate-Specific Antigen. People don't think about this enough, but immediately after ejaculation, semen actually clots into a thick, gel-like substance to keep it from washing away. This is where PSA enters the picture. It acts as a molecular pair of scissors, liquefying the gel so the sperm can actually swim toward their target. Yet, this enzyme has become a double-edged sword in modern medicine. In 1994, the FDA approved the PSA blood test as a screening tool for prostate cancer, a milestone that completely transformed oncology but also ushered in an era of massive over-diagnosis. A spiked PSA score can mean a lethal tumor, sure, but it can just as easily mean you rode your bicycle too far on a Sunday morning or had a mild, unnoticed infection.
The Neurological Connection
And then there is the nerve network. The prostate is surrounded by a delicate web of cavernous nerves that are directly responsible for triggering erections. Because these microscopic fibers hug the outer capsule of the gland so closely, any surgical intervention becomes a high-stakes game of operation. One wrong millimeter and that changes everything for a man's sex life.
Life Without a Prostate: Radical Prostatectomy and the Fallout
The issue remains: what happens when we decide to rip the whole thing out? When a biopsy reveals an aggressive cancer, a surgeon might perform a radical prostatectomy—the complete surgical removal of the gland. I have talked to patients who assumed life would simply return to normal afterward, except that they would stop worrying about cancer. We are far from it. Once the prostate is gone, a man experiences what is known as a dry orgasm; the sensation of pleasure remains intact, but there is absolutely no fluid produced. It is a bizarre, jarring sensory shift that takes considerable psychological adjustment.
The Structural Reconstruction
Because the surgeon has to cut the urethra to remove the gland, they have to pull the bladder down and sew the remaining pipe back together, a delicate procedure known as a vesicourethral anastomosis. During the healing process, control over the urinary sphincter is severely compromised. Statistics show that up to twenty percent of men still require pads for urinary incontinence a full year after surgery. It turns out that the prostate acted as a physical backstop, helping to hold back urine under pressure. Remove that structural support, and the bladder suddenly has to relearn how to hold its contents when you laugh, cough, or lift a box of groceries.
The Evolution of Treatment: Why Total Removal is No Longer the Only Option
For decades, the medical establishment treated the prostate like a ticking time bomb—if it showed signs of trouble, the default response was often to cut it out or blast it with radiation. Fortunately, the paradigm is shifting toward more nuanced approaches. In places like the Mayo Clinic in Rochester, Minnesota, doctors are increasingly championing active surveillance for low-risk tumors, recognizing that many men will die with prostate cancer rather than from it. Why endure the life-altering side effects of surgery for a microscopic speck of cancer that might take thirty years to move a millimeter?
High-Tech Alternates to the Scalpel
Moreover, modern technological interventions are completely rewriting the playbook for non-cancerous enlargement. Instead of carving out tissue, urologists now utilize procedures like Holmium Laser Enucleation or water jet ablation, which precisely target the obstructive transition zone while leaving the outer shell and those critical erection nerves completely untouched. As a result: recovery times have plummeted from weeks to days, allowing men to preserve both their continence and their dignity without resorting to organ amputation.
Common mistakes and myths surrounding the gland
The confusion between size and malignancy
Size does not equal cancer. Let's be clear: a walnut-sized organ ballooning to the volume of a tennis ball feels alarming, yet this hypertrophic expansion usually represents benign prostatic hyperplasia rather than an aggressive oncological threat. Millions of individuals assume that severe urinary hesitation dictates a terminal diagnosis. The problem is that benign cellular proliferation blocks the urethra mechanically, which explains why a massive non-cancerous growth causes immense discomfort while a tiny, silent tumor produces zero immediate symptoms. Doctors routinely encounter patients who are paralyzed by fear over a high prostate-specific antigen count, neglecting the reality that simple inflammation or recent sexual activity spikes these metrics drastically. Do men need a prostate to function normally? They certainly do, but they often misinterpret its mechanical signals completely.
The assumption of immediate surgical necessity
Panic frequently drives hasty medical decisions. When a physician flags a nodule, the immediate visceral reaction involves demanding total eradication of the offending tissue. Except that modern urological protocols vehemently advocate for active surveillance in low-risk scenarios. Knife-happy approaches can cause permanent structural damage. Data indicates that roughly fifty percent of low-grade localized tumors never advance to threaten a patient's longevity during their natural lifetime. But instead of breathing a sigh of relief, patients rush into operating rooms, trading a slow-moving, harmless condition for immediate pelvic floor dysfunction. Overtreatment remains a massive systemic hurdle in modern urology.
The neurological cost of radical intervention
The hidden web of pelvic potency
Surgeons talk endlessly about margins, though the architectural reality beneath the bladder is far more intricate than basic oncology maps suggest. Microscopic cavernosal nerve bundles, which dictate erectile functionality, hug the capsule of this gland with terrifying proximity. Can a scalpel truly separate them without leaving a trace of collateral damage? (Medical robots claim precision, but human biology rarely conforms to perfect straight lines). If oncological survival demands total removal, the psychological price tag involves redefining intimate wellness from scratch. The issue remains that while the primary tumor vanishes, the complex neural highway responsible for spontaneous vascular engorgement is permanently disrupted, leaving men to navigate a sudden, starkly altered physical landscape.
Frequently Asked Questions
Does removing the organ mean an absolute end to a man's sex life?
No, because intimacy evolves rather than disappears after radical treatment. While direct mechanical emission becomes impossible due to the structural severance of the seminal vesicles, the neurological capacity for orgasmic sensation resides primarily in the pelvic nerves and brain. Statistically, clinical trials demonstrate that between forty to sixty percent of patients recover sufficient erectile capacity for intercourse within twenty-four months post-surgery, provided nerve-sparing techniques were successfully deployed. Modern urologists utilize vacuum devices, penile injections, and targeted rehabilitation therapies to aggressively stimulate blood flow during the recovery phase. As a result: physical pleasure persists, albeit via a completely dry ejaculatory experience.
Can lifestyle modifications realistically prevent the need for prostate surgery later in life?
Dietary overhauls cannot alter genetic predispositions entirely, yet targeted behavioral modifications significantly reduce the severity of lower urinary tract symptoms. Incorporating specific micronutrients like lycopene alongside zinc helps stabilize cellular metabolic pathways within the local tissue environment. Clinical research tracking large cohorts reveals that a body mass index maintained under twenty-five reduces the risk of symptomatic benign enlargement by approximately twenty-eight percent compared to obese demographics. Regular cardiovascular exercise mitigates pelvic congestion, optimizing vascular perfusion throughout the lower abdomen. In short, while wellness habits fail to guarantee absolute immunity from age-related changes, they actively downregulate chronic inflammatory markers that accelerate glandular swelling.
How does a man know if his urinary difficulties stem from infection or structural growth?
Distinguishing between acute prostatitis and chronic mechanical obstruction requires analyzing the velocity of symptom onset. Bacterial infections arrive with blinding speed, accompanied by systemic markers like a sudden fever, burning during urination, and deep perineal pain. Structural issues, conversely, develop over decades, gradually narrowing the urinary channel until the bladder detrusor muscle weakens from fighting constant resistance. A standard urological evaluation employs a simple flowmetry test to chart the exact voiding velocity, where a peak flow rate below ten milliliters per second strongly points toward long-term anatomical blockage rather than acute inflammation. Precise diagnosis prevents the catastrophic misuse of antibiotics for non-bacterial structural ailments.
An unvarnished verdict on male anatomical necessity
We must abandon the archaic notion that this pelvic organ is merely a ticking time bomb waiting to sabotage aging bodies. It remains a sophisticated biological engine driving reproductive capability and localized fluid dynamics, demanding proactive preservation rather than casual surgical elimination. Embracing aggressive intervention at the first sign of fluctuation is a flawed strategy that frequently trades longevity for a severely compromised quality of life. The medical community needs to prioritize nuanced, organ-sparing treatments that respect the delicate neurological framework governing the male pelvis. Informed active surveillance must become the gold standard for management, preventing unnecessary trauma to a system that requires balance to thrive. Ultimately, saving the man shouldn't require the thoughtless destruction of his foundational anatomy.