The Structural Crossroads: Decoding When the Prostate Forces a Surgeon’s Hand
Let us be completely honest here. The prostate is an anatomical design flaw—a walnut-sized gland wrapped snugly around the urethra that, as decades pass, almost inevitably expands. But expansion alone is not a ticket to the operating theater. The thing is, we must separate the slow-burning fuse of benign enlargement from the silent, chaotic mutation of oncological cells. I have watched patients panic over a mildly elevated Prostate-Specific Antigen (PSA) test, assuming they would be on an operating table by the weekend. We are far from it.
The Urethral Chokehold of Benign Prostatic Hyperplasia
In the benign realm, size does not dictate surgery. Instead, the true metric is functional failure. You can have a massively enlarged prostate that causes fewer issues than a smaller, strategically positioned nodule that pinches the bladder neck like a kinked garden hose. When the American Urological Association (AUA) Symptom Index score climbs past 20, or when a man experiences acute urinary retention—the sudden, agonizing inability to pass even a drop of urine—the conversation shifts dramatically from lifestyle adjustments to surgical planning.
The Oncological Threshold: When Watching and Waiting Ends
Cancer operates by an entirely different set of rules. Here, determining at what stage is prostate surgery required relies heavily on Risk Stratification Matrices rather than how many times you wake up to use the bathroom at night. Active surveillance is the modern gold standard for low-risk, indolent tumors (Gleason Score 6). Yet, the moment a routine biopsy at a clinic like the Mayo Clinic detects a shift to Gleason Grade Group 2 or 3 (Gleason 3+4=7 or 4+3=7), the clinical landscape alters instantly. That changes everything, because those numbers signify a tumor that has lost its predictable, lazy nature and is preparing to migrate.
The Oncological Timeline: Pinpointing the Radical Prostatectomy Trigger
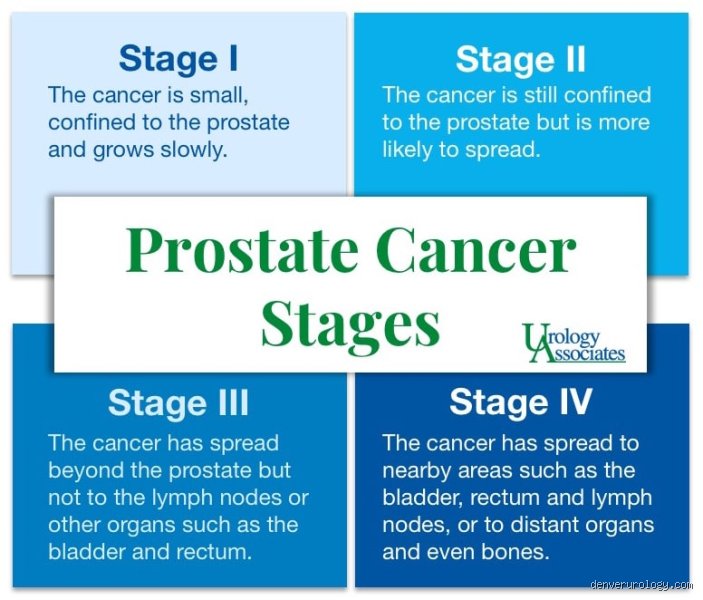
When dealing with adenocarcinoma, urologists utilize the tumor, node, metastasis (TNM) staging system alongside PSA serum levels to calculate the exact window for a radical prostatectomy. The sweet spot for surgical efficacy rests almost exclusively within stages T1c through T2c. These represent tumors that are entirely confined within the fibrous sheath of the prostate gland. Why is this specific window so paramount? Because once the malignant cells violate that boundary—moving into Stage T3 where they infiltrate the seminal vesicles or the bladder neck—the probability of achieving clear surgical margins drops precipitously.
The Mathematical Breaking Point: PSA Velocity and Gleason Scores
Consider the raw metrics that drive these decisions. A patient presenting with a PSA density greater than 0.15 ng/ml/cc combined with a genomic classifier score—such as the Decipher prostate cancer test—indicating high genomic risk cannot afford the luxury of watchful waiting. Where it gets tricky is the interpretation of PSA velocity; a sudden doubling of PSA within 12 months, even if the absolute number remains below the traditional 4.0 ng/mL threshold, frequently serves as the primary catalyst for shifting a patient from active surveillance straight to the pre-operative schedule. It is a numbers game where hesitation carries a massive penalty.
The T3 Dilemma: When Surgery Requires Neoadjuvant Reinforcements
But what happens if a patient crosses into Stage T3 asymptomatic illness? Some institutional guidelines, notably those from the European Association of Urology (EAU), suggest that surgery at this advanced junction should rarely be a standalone treatment. Instead, it becomes part of a multimodal assault. If the tumor has crept into local tissues, a surgeon might still operate, but only with the explicit understanding that salvage radiation therapy will likely follow. It is a aggressive gamble to debulk the primary tumor site before systemic spread locks in.
The Benign Breaking Point: When BPH Transcends Medication
Switching gears to non-malignant disease, the question of at what stage is prostate surgery required is answered not by cellular pathology, but by mechanical failure and secondary organ damage. Urologists typically exhaust the pharmaceutical arsenal first. Patients are routinely started on 5-alpha reductase inhibitors like finasteride to shrink the tissue, alongside alpha-blockers like tamsulosin to relax the bladder neck. But these drugs are temporary fixes, not cures.
The Cascade of Bladder Decompensation
The issue remains that long-term urinary obstruction induces irreversible changes in the bladder wall detrusor muscle. Because the bladder must pump harder and harder against the prostatic blockage to expel urine, it undergoes muscular hypertrophy, developing thick ridges known as trabeculations. If you leave this unaddressed, the bladder eventually loses its contractility entirely—a condition known as an atonic bladder. Once the bladder dies, removing the prostate won't fix your plumbing; hence, surgeons prefer to intervene well before this point of no return is reached.
The Absolute Surgical Mandates in Benign Disease
There are four absolute, non-negotiable indications that a BPH patient has reached the stage where surgery is mandatory. First, recurrent episodes of acute urinary retention requiring emergency catheterization. Second, persistent gross hematuria (visible blood in the urine) caused by the rupture of fragile, engorged veins stretching over the enlarged prostate. Third, bladder calculi (stones) forming due to chronic urinary stasis. Finally, the most dangerous trigger: bilateral hydronephrosis, where backed-up urine creates high pressure in the ureters, causing renal insufficiency and threatening total kidney failure.
Therapeutic Evolution: Comparing the Surgical Triggers Across Modalities
The criteria for when a patient needs surgery have shifted due to the rise of minimally invasive technologies. Twenty years ago, an open retropubic prostatectomy was a brutal, bloody affair that made both doctors and patients delay the intervention as long as humanly possible. Today, the threshold for surgery has actually lowered because the morbidity of the procedures themselves has plummeted.
The Minimalist Shift in Benign Interventions
We see this clearly with the adoption of procedures like Holmium Laser Enucleation of the Prostate (HoLEP) and robotic-assisted surgeries. Because a HoLEP can safely core out adenomas weighing over 100 grams without a single external incision, patients no longer need to wait until they are in renal duress to qualify. People don't think about this enough: early intervention with a low-morbidity procedure often preserves sexual and urinary function far better than waiting until the anatomy is utterly distorted by decades of chronic inflammation.
The Robotic Precision Era in Oncology
In oncology, the widespread adoption of the da Vinci surgical system has similarly redefined our timeline. With superior visualization of the delicate cavernous nerves responsible for erectile function, surgeons are more willing to recommend a robotic-assisted laparoscopic prostatectomy (RALP) for younger, healthier men in the early phases of Stage T2 disease. Except that this technological leap creates a psychological trap—the temptation to cut out low-risk tumors that would likely never kill the patient in their lifetime remains a contentious issue within the urological community, illustrating that just because we can operate elegantly does not mean we always should.
Common Mistakes and Misconceptions Regarding Urological Intervention
The "Cancer Equals Immediate Scalpel" Fallacy
Panic drives decisions. When a biopsy reveals malignant cells, the knee-joint reaction is often demanding immediate eradication. The problem is, prostate surgery required at this exact moment might actually represent overtreatment. Low-risk, localized tumors frequently mimic a sleeping dog; waking it up with a radical prostatectomy introduces risks like erectile dysfunction or urinary incontinence without necessarily extending your lifespan. Experts now advocate for active surveillance in up to sixty percent of low-risk patients, turning the knife into a weapon of last resort rather than a first line of defense.
Conflating BPH Severity with Surgical Necessity
An enlarged gland does not automatically mandate an operating room. Many men assume that a massive prostate equals inevitable resection. Except that, the mechanical volume of the tissue matters far less than the actual restriction imposed on the urethra. A relatively small adenoma can cause complete urinary retention, while a mammoth-sized organ might only provoke mild, manageable symptoms. Basing your entire treatment trajectory solely on ultrasound dimensions is a clinical blunder; we must look at functional impairment instead.
Ignoring the Window of Bladder Compensation
Waiting too long is just as treacherous as rushing in. Patients frequently tolerate escalating misery, believing they are being stoic. But what happens to the detrusor muscle during this prolonged struggle? It hypertrophies, weakens, and eventually undergoes irreversible fibrotic changes. If you delay intervention until the bladder loses its contractile power, removing the prostate obstruction will not fix the underlying urinary stasis. At what stage is prostate surgery required? It is required before the bladder sacrifices itself to overcome the blockage.
The Urodynamic Secret: What Your Surgeon Might Not Mention
The Hidden Metrics of Detrusor Pressure
Let's be clear: a standard uroflowmetry test only scratches the surface. It measures output, not the internal workload required to produce that output. True expert guidance relies on advanced multichannel urodynamic studies to isolate the pressure-flow relationship. Why do we care? Because a low flow rate could mean an obstructed prostate, or it could mean a dying bladder muscle. Operating on the latter yields disastrously poor outcomes, which explains why sophisticated pressure profiling is the unsung hero of surgical planning.
The Microvascular Reality of Recovery
We often discuss nerve-sparing techniques as a binary outcome, yet tissue perfusion dictates the true success of these procedures. Microsurgical preservation of the accessory pudendal arteries determines whether a patient regains potency within twelve months post-op. If these tiny vessels are already compromised by smoking or diabetes, even the most meticulous robotic dissection faces a steep uphill battle. It is an intricate anatomical gamble that demands realistic expectations from both the patient and the urologist.
Frequently Asked Questions
Does a PSA velocity increase mean prostate surgery required immediately?
An isolated spike in Prostate-Specific Antigen levels triggers immense anxiety, yet it rarely justifies an immediate trip to the operating theater. A velocity increase exceeding 0.75 nanograms per milliliter per year certainly warrants a secondary investigation, such as a multiparametric MRI or a targeted transperineal biopsy. However, benign conditions like acute prostatitis, vigorous exercise, or recent sexual activity can easily skew these biochemical metrics. Urologists typically require a sustained, confirmed trajectory over at least three distinct readings before altering a therapeutic roadmap. Therefore, acceleration merely dictates deeper diagnostic scrutiny, not an automatic surgical mandate.
What is the maximum post-void residual volume allowed before operating?
While there is no universally carved-into-stone threshold, a consistent post-void residual volume exceeding two hundred milliliters serves as a major red flag for clinical intervention. Accumulating this much stagnant urine within the vesicle creates a perfect breeding ground for recurrent bacterial infections and bladder calculi. More alarmingly, this persistent volume generates backward hydrostatic pressure that can silently damage the kidneys, leading to post-renal azotemia. When retention reaches this critical volume alongside failing medical therapy, the clinical consensus shifts rapidly toward mechanical debulking. Consequently, monitoring this specific metric prevents silent, irreversible upper urinary tract degeneration.
How does age influence the decision to undergo a radical prostatectomy?
Chronological age is vastly subordinate to biological longevity when determining surgical candidacy. Generally, a patient should possess a minimum life expectancy of ten to fifteen years to reap the survival benefits of a radical prostatectomy for localized cancer. For an otherwise healthy seventy-five-year-old gentleman, the procedure remains a highly viable, life-extending option. Conversely, a sixty-year-old individual burdened by severe cardiovascular disease might derive far more harm than benefit from general anesthesia and pelvic surgery. (Health optimization always supersedes the birth certificate date). Thus, the modern urological approach focuses entirely on frailty indexes and comorbidity profiling rather than arbitrary age limits.
A Definitive Stance on the Surgical Threshold
The decision to operate on the prostate should never be viewed as an inevitable consequence of aging or an automatic response to a laboratory value. We must draw a hard line against the pervasive medical trend of treating images and laboratory reports rather than the living, breathing patient. At what stage is prostate surgery required? It becomes mandatory the precise moment objective functional decline outpaces the protective capacity of conservative management, threatening renal integrity or destroying daily quality of life. Relying blindly on pharmaceuticals to delay the inevitable often leaves patients with a permanently damaged bladder. As a result: true urological expertise lies in identifying that fleeting therapeutic window where intervention provides maximum long-term relief with minimal structural collateral damage. Do not let fear dictate the timing, but do not let stubborn avoidance ruin your long-term prognosis either.