Common mistakes and misconceptions
The myth of the single culprit
Confusing incidence with mortality
Let's be clear: having the most frequent bouts of illness does not automatically equal having the most open graves. Western discussions often lump these two metrics together, creating massive statistical confusion. For instance, data indicates that Madagascar recently registered a staggering age-standardized incidence rate exceeding 199,000 cases per 100,000 individuals for childhood gastrointestinal infections. Yet, does it hold the highest mortality crown? No. That grim title shifts elsewhere because a country might have frequent outbreaks but possess just enough oral rehydration therapy access to prevent absolute dehydration. We must separate the sheer volume of sick days from the ultimate, fatal outcomes.
Little-known aspects and expert advice
The deadly math of absolute population weight
The problem is that our brains perceive risk through percentages, whereas human suffering happens in absolute numbers. When evaluating the global landscape of diarrheal disease transmission, smaller nations frequently show the highest individual probability of death. Consider the Central African Republic, where childhood mortality from these conditions has peaked near 6.9 deaths per 1,000 children. That is an astronomical rate. But because its total population is relatively small, it results in roughly 4,100 yearly child fatalities. In contrast, Nigeria exhibits a mortality rate that is less than half of that percentage, yet its massive population density translates to over 104,000 children dying annually. Which baseline dictates our international aid priorities? The tension between per-capita severity and total body counts remains a massive geopolitical debate for global health funders.
Aggressive rehydration is the true frontline
Forget complex pharmaceutical silver bullets. Experts know that the absolute best weapon against this global killer is a humble, low-tech mixture of clean water, salt, and glucose. If you want to crash the mortality rates in high-burden zones, you do not wait for expensive sewage treatment plants to be built over several decades. You distribute simple oral rehydration salts alongside zinc supplements immediately. The issue remains that in critical parts of sub-Saharan Africa and South Asia, only about one in three children receives this basic life-saving protocol. Changing that dynamic requires logistical willpower rather than medical breakthroughs.
Frequently Asked Questions
Which country currently records the highest death rate from diarrheal diseases?
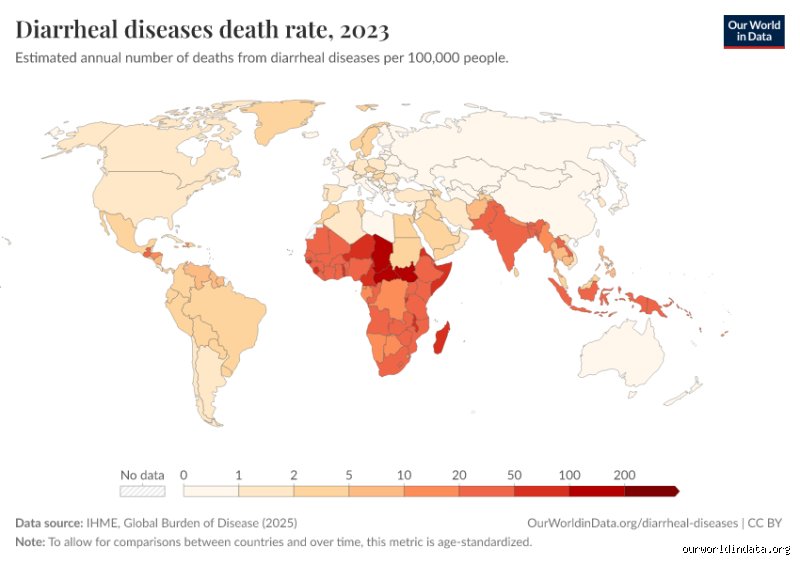
According to comprehensive epidemiological metrics tracked by global health institutions, Chad ranks first globally in age-standardized death rates for childhood diarrheal diseases. The nation exhibits an alarming rate of approximately 233.98 deaths per 100,000 individuals, alongside the highest disability-adjusted life years rate recorded anywhere on the planet. This devastating reality is driven by a severe lack of protected water sources and structural health systems. While other nations might see more total cases due to larger populations, Chad represents the most lethal environment for young children experiencing severe gastrointestinal distress.
Why do sub-Saharan Africa and South Asia consistently bear the highest global burden?
The concentration of these diseases in these specific zones is a direct consequence of intersecting environmental and socioeconomic challenges. High population density combined with inadequate fecal sludge management allows waterborne pathogens to spread rapidly through community resources. Statistics show that these two regions account for the vast majority of global child deaths from dehydration, primarily due to low coverage of essential interventions. Because historical infrastructure investments have failed to keep pace with rapid urbanization, millions of families still rely on unimproved water supplies daily.
Can climate change alter which country has the highest diarrhea rate?
Escalating global temperatures and erratic weather patterns are already actively shifting the boundaries of high-transmission zones. Increased flooding events routinely overwhelm fragile sanitation networks, instantly contaminating shallow wells and municipal water supplies with human waste. Conversely, severe droughts force desperate communities to rely on stagnant, highly concentrated water sources teeming with pathogenic bacteria. As a result: hyper-local spikes in waterborne illnesses are becoming increasingly common across areas that previously enjoyed seasonal stability.
Engaged synthesis
We can no longer treat global dehydration as an inevitable byproduct of tropical geography. The data proves that the answer to what country has the highest diarrhea rate is determined entirely by political choice and infrastructure funding. It is an absolute ethical failure that over 440,000 children under the age of five still perish annually from a condition that costs pennies to treat. We must stop hiding behind complex medical jargon and admit that this is a straightforward crisis of poverty and structural neglect. Funding must be aggressively redirected away from bureaucratic red tape and poured directly into localized water security and basic rehydration distribution. Until the international community treats clean drinking water as an uncompromisable human right, our global health metrics will remain stained by these entirely preventable deaths.