The Hidden Mechanics of Fluid Balance and Why Your Stomach Fails
Most people view digestion as a simple conveyor belt. The reality is far more chaotic, involving a massive fluid exchange that would shock the average person. Every single day, your gastrointestinal tract processes roughly 9 liters of fluid, a staggering amount considering you only drink a fraction of that volume. The vast majority—about 8.5 liters—is aggressively reabsorbed by the small intestine and colon, leaving a mere 100 to 200 milliliters to be excreted in normal stool. Where it gets tricky is when the delicate balance of epithelial cells is disrupted by pathogens or toxins.
The Delicate Barrier: Enterocytes Under Siege
Your gut lining consists of a single layer of cells called enterocytes. These microscopic workhorses use a complex network of sodium-glucose cotransporters to pump water back into your bloodstream. But what happens when a rogue strain of Escherichia coli or a heavy dose of magnesium ions disrupts this cellular machinery? The system reverses. Instead of absorbing, the cells either secrete water or allow it to bypass the filtration system entirely. Honestly, it's unclear why some people's microbiomes can withstand a massive influx of pathogens while others collapse at the slightest hint of a tainted salad, but the resulting fluid shift remains identical.
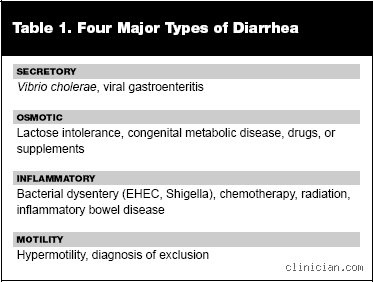
Type 1: Secretory Diarrhea and the Relentless Cellular Pump
Think of secretory diarrhea as a faucet that has been completely stripped of its handle. In this state, your intestinal walls actively pump electrolytes and water into the lumen of the gut, regardless of whether you have eaten anything or not. Fasting does not stop it. Because the secretion is driven by internal cellular signals—often triggered by bacterial toxins like the ones produced during a Vibrio cholerae outbreak—the diarrhea persists even if you consume absolutely nothing for 24 hours. This is the hallmark feature that sets it apart from dietary issues.
The Cyclic AMP Cascade: How Toxins Hijack Your Biology
The molecular villain here is usually an overstimulation of intracellular signaling molecules, specifically cyclic adenosine monophosphate, or cAMP. When a pathogen binds to the enterocyte, it forces the cell to permanently open its chloride channels. And because water always follows salt, a massive torrent of hydration leaves your blood vessel walls and floods your gut, leading to the classic, high-volume "rice-water" stools. I argue that secretory diarrhea is the most dangerous of the four categories because of how rapidly it induces severe, life-threatening dehydration. During the infamous 1991 cholera epidemic in Peru, patients were losing up to 20 liters of fluid per day, illustrating just how violently this mechanism can overwhelm human physiology.
Non-Infectious Triggers: When Your Own Hormones Turn Rogue
But microbes are not the sole culprits behind this relentless pumping action. Certain rare neuroendocrine tumors, such as VIPomas, secrete vast amounts of Vasoactive Intestinal Peptide, which mimics the exact same cAMP activation. It is a terrifying thought—your own endocrine system mimicking a tropical pathogen. Certain laxatives, like senna or ricinoleic acid found in castor oil, also induce this secretory state by irritating the mucosa. You might think you are doing a simple colon cleanse, but you are actually forcing a cellular-level evacuation that changes everything.
Type 2: Osmotic Diarrhea and the Danger of Unabsorbed Solutes
Osmotic diarrhea operates on a completely different principle, one that is entirely dependent on what you put into your mouth
Common mistakes and misconceptions
The dehydration trap
You probably think chugging pure water is the ultimate cure when dealing with the four types of diarrhea. Except that it is not. Guzzling massive quantities of plain H2O actually dilutes your remaining blood electrolytes, a dangerous physiological blunder known as hyponatremia. When your gut undergoes severe fluid loss, it sheds sodium, potassium, and chloride at an alarming velocity. To fix this, medical professionals rely on Oral Rehydration Salts (ORS) which utilize a precise 1:1 molar ratio of glucose to sodium to force the intestinal walls to absorb fluids. Let's be clear: relying solely on tap water can worsen your recovery timeline by prolonging intestinal transit time.
The immediate anti-motility reflex
Stopping the flow immediately seems logical. Why suffer? Yet, swallowing anti-diarrheal medications like loperamide the second your stomach rumbles is frequently a terrible mistake. If your illness stems from an invasive bacterial pathogen such as Salmonella or Shigella, your body is actively using hyper-motility to flush out these micro-organisms. By artificially paralyzing your bowel walls with medication, you trap the bacteria and their metabolic toxins inside your colon. The issue remains that this can precipitate toxic megacolon, a rare but life-threatening complication where the large intestine swells massively. Did you really want to keep those toxins trapped inside your gastrointestinal tract?
The bland diet myth
For decades, pediatricians and general practitioners shoved everyone toward the strict BRAT diet, which stands for bananas, rice, applesauce, and toast. Modern gastroenterology has shifted away from this restrictive regimen. This highly restrictive approach lacks sufficient protein and micronutrients, which actually delays the cellular repair of the damaged intestinal mucosa. Clinical trials indicate that continuing a regular, age-appropriate diet speeds up enterocyte regeneration, provided you skip excessive fats and concentrated sugars.
A hidden driver: The bile acid factor
The overlooked hepatic link
Most patients focus entirely on bacteria or food intolerances when diagnosing the four types of diarrhea, completely ignoring their own liver metabolism. Bile acid malabsorption (BAM) is a frequently misdiagnosed condition that accounts for approximately twenty-five percent of chronic diarrhea cases worldwide. Normally, your terminal ileum reabsorbs around ninety-five percent of bile acids synthesized by the liver. When this mechanism fails, excess bile acids enter the colon, where they act as potent natural laxatives by stimulating secretory pathways. As a result: patients endure years of bloating and explosive liquid stools, mistakenly labeled as irritable bowel syndrome, because doctors fail to measure fecal bile acid excretion. This specific pathophysiological pathway requires a totally unique treatment strategy, utilizing bile acid sequestrants like cholestyramine rather than standard antibiotics or probiotics.
Frequently Asked Questions
How long do the four types of diarrhea typically last before requiring clinical intervention?
Acute episodes, usually driven by viral infections or toxic food poisoning, generally resolve spontaneously within forty-eight to seventy-two hours without specific pharmacological intervention. However, if the loose stools persist past fourteen days, the condition enters the persistent phase, and beyond thirty days, it is officially classified as chronic. Epidemiological data indicates that roughly five percent of the global population suffers from chronic gastrointestinal hyper-motility at any given time. You should absolutely seek immediate emergency medical evaluation if you detect a fever exceeding 102 degrees Fahrenheit or notice dark blood in your stool.
Can psychological stress directly trigger secretory or osmotic bowel movements?
Yes, the brain-gut axis exerts massive control over your digestive tract through a dense neural network called the enteric nervous system. When you experience intense acute anxiety, your brain releases high levels of corticotropin-releasing factor, a hormone that stimulates colonic mast cells to release histamine and serotonin. These chemical messengers rapidly accelerate colonic transit time while simultaneously increasing mucosal secretion, mimicking the exact symptoms of osmotic imbalances. But your emotional state cannot induce true inflammatory tissue destruction, meaning stress-induced episodes never contain fecal calprotectin, a biomarker for cellular damage. In short, your mind can easily liquefy your stool, though it will not cause structural ulcerations in your colon wall.
Are routine probiotic supplements effective across all variations of this condition?
The problem is that the public views probiotics as a magical panacea for every single stomach ailment. Clinical efficacy is highly strain-specific, meaning a bacterial strain that pacifies antibiotic-associated loose stools might do absolutely nothing for secretory cholera. For example, extensive clinical meta-analyses show that only specific strains like Lactobacillus rhamnosus GG and Saccharomyces boulardii reduce the duration of acute viral gastroenteritis by an average of twenty-four hours. Buying a random, generic supermarket yogurt or a poorly formulated pill is mostly a waste of your money. We must acknowledge the limits of current commercial microbiology, as stuffing billions of random bacteria into an already inflamed, hyper-potent ecosystem rarely yields predictable therapeutic outcomes.
A definitive stance on intestinal health
Stop treating your gut like a simple, broken plumbing pipe that just needs a temporary plastic plug. The complex existence of the four types of diarrhea proves that your digestive tract is a sophisticated, highly reactive immune organ reacting to distinct physiological insults. Treating an inflammatory bacterial infection the exact same way you treat a mild lactose-induced osmotic imbalance is an exercise in medical futility. We need to abandon the simplistic culture of self-medicating with over-the-counter blockers every time our digestion falters. Demanding precise diagnostic testing, rather than settling for vague lifestyle labels, is the only real way to regain permanent metabolic control. Your intestinal tract deserves a strategy based on rigorous pathology, not convenient guesswork.