The Messy Reality of Gastrointestinal Upset and Fluid Loss
Diarrhea is not just an inconvenience; it is a chaotic physiological defense mechanism. When a pathogen—say, the notorious Campylobacter jejuni strain tracked during the infamous 2010 outbreak in Ohio—invades your digestive tract, the intestines shift into overdrive. The mucosal lining flushes out the invaders, resulting in massive fluid loss. People assume the biggest threat is the bugs themselves. The thing is, the real danger is rapid, systemic dehydration.
Decoding Hypertonic Versus Hypotonic Liquids in Your Gut
Your intestinal walls behave like a strict border control agent operating via osmosis. If you drink a highly concentrated, hypertonic brine, you create a massive osmotic gradient that pulls water straight out of your vascular system and into the bowel lumen. What does that mean for your gut? It means instant disaster. A high-sodium fluid backfires spectacularly by drawing water into the intestines rather than absorbing it. Yet, if the fluid is hypotonic—lower in solute concentration than your blood—the opposite occurs. The fluid enters the tissue, which explains why the exact concentration of your beverage dictates whether your bathroom trips will cease or double in frequency.
What Happens When Sodium Levels Spike Outside the Cells
Because the body constantly chases equilibrium, flooding your stomach with random kitchen salt solutions triggers cellular panic. The extracellular space becomes dense with sodium ions, forcing intracellular water to escape to balance the pressure. This can lead to hypernatremia, a dangerous state of electrolyte imbalance. Honestly, it is unclear why so many wellness influencers still recommend random saltwater flushes when the cellular math simply does not add up.
The Molecular Machinery of Absorption and the Sodium-Glucose Co-Transporter
Here is where it gets tricky for the average person trying a home remedy. Your intestinal cells possess tiny molecular pumps called SGLT-1 co-transporters. These microscopic gateways are remarkably stubborn. They refuse to allow sodium to cross the cellular membrane unless a molecule of glucose is standing right next to it. But if you provide both simultaneously? That changes everything.
Why Plain Salted Water Fails Without a Sugar Escort
Imagine the SGLT-1 transporter as a nightclub bouncer who only admits couples. Plain salt water is just a line of single sodium ions waiting outside the club. Because there is no glucose present to unlock the gate, the sodium remains trapped in the intestinal tract, pulling more water toward itself and aggravating the irritation. I have seen amateur survivalists claim that drinking sea salt solutions keeps them hydrated during stomach bugs, but we are far from it. Without a precise 1:1 molar ratio of glucose to sodium, the mixture passes through you unused.
The World Health Organization Shift and the 1971 Breakthrough
During the devastating 1971 cholera outbreak in refugee camps in West Bengal, medical teams faced a catastrophic shortage of intravenous fluids. Dr. Dilip Mahalanabis introduced an experimental oral rehydration solution that combined specific quantities of salt and glucose. It was a staggering success, slashing mortality rates from 30% down to less than 3%. This historic intervention proved that utilizing the SGLT-1 pathway via oral fluids could match the efficacy of an IV drip. As a result: the World Health Organization standardized the formula, eventually optimizing it into the modern low-osmolarity ORS used globally today.
Analyzing the Dangers of Homemade Brines and Sea Salt Mixes
The temptation to stir a teaspoon of pink Himalayan sea salt into a warm mug of water during a bout of illness is strong. The issue remains that human hands are notoriously bad at measuring microscopic chemical ratios without laboratory scales. A standard teaspoon of table salt contains roughly 2,300 milligrams of sodium, a dose that can shock an already inflamed colon.
The Fine Line Between Rehydration and Osmotic Purging
When you brew a random homemade solution, you are essentially gambling with your bowel transit time. If the mix is even slightly too concentrated, it initiates an osmotic purge. Did you know that some colonoscopy prep solutions are literally just concentrated salt formulations designed to empty the bowels completely? You might accidentally replicate this exact mechanism in your kitchen while trying to do the opposite. And if your kidneys are already stressed from fluid loss, processing that excess sodium places an immense burden on your renal filtration system.
Why Gourmet Salts Do Not Help Your Intestines
People often argue that unrefined grey salt or Celtic sea salt contains trace minerals that protect the stomach. While those variants do possess minor amounts of magnesium and potassium, their core composition is still sodium chloride. The gut does not care if your salt was harvested from a pristine French flat or an industrial mine; it only reacts to the ionic concentration hitting the epithelial cells.
Evaluating Modern Rehydration Alternatives Against Traditional Remedies
When we look at modern options compared to traditional remedies, standard tap water with salt ranks near the bottom for treating acute diarrhea. Commercial sports drinks are not much better, given their notoriously high fructose content. The excess sugar in a standard sports beverage can pull water into the gut just as easily as excess salt does, creating a different pathway to the exact same miserable result.
The Compositional Breakdown of Effective Rehydration Solutions
To understand what actually works, we have to look at the precise architecture of a standard low-osmolarity ORS packet. These packets typically combine 2.6 grams of sodium chloride, 2.9 grams of trisodium citrate dihydrate, 1.5 grams of potassium chloride, and 13.5 grams of anhydrous glucose per liter of water. This specific combination yields an osmolarity of 245 mOsm/L. This number is vital because it sits perfectly below the osmolarity of human plasma, allowing the damaged intestinal lining to absorb every single drop of fluid efficiently without forcing the kidneys to overwork.
Common Mistakes and Misconceptions Regarding Oral Rehydration
People often panic when gastrointestinal distress strikes. They run to the kitchen. They grab the nearest container of table salt, dump a random spoonful into a glass of tap water, and chug it down. This amateur chemistry is remarkably dangerous. Do you really think your internal organs enjoy processing random concentrations of sodium? The problem is that guessing the ratio completely destroys the osmotic balance in your gut. Instead of halting the fluid loss, a hypertonic saline mixture draws even more water from your bloodstream into your intestinal lumen. As a result: your symptoms worsen drastically.
The Lethal Myth of the Ocean Cure
Some individuals genuinely believe that natural seawater possesses magical healing properties for digestive ailments. Let us be clear: drinking ocean water will cause severe, life-threatening dehydration. Sea water has a salinity of roughly 35 grams per liter. Your kidneys require more freshwater than that to excrete the excess salt, meaning you will rapidly deplete your remaining fluid reserves. Stranded sailors die from this exact mistake, yet internet forums occasionally resurrect it as a holistic remedy. It fails miserably because the high magnesium and sulfate content in natural brine acts as a potent laxative.
Chugging Large Volumes Too Quickly
When you are desperate to replace lost fluids, your immediate instinct is to gulp down an entire quart of liquid in one sitting. Your hyper-reactive, inflamed stomach will immediately reject this sudden volume. Vomiting ensues. Because your gastric lining is already highly sensitive during an infection, you must administer liquids in tiny, frequent sips. Think teaspoons, not pint glasses. Flooding the digestive tract triggers the gastrocolic reflex, which promptly forces your bowels to evacuate whatever contents remain, rendering your rehydration efforts completely useless.
The Hidden Impact of Zinc Co-Administration
Medical professionals look beyond simple sodium and water metrics. While everyone argues over whether does salt water stop diarrhea, the global health community focuses heavily on micronutrient synergy. Except that most people completely ignore zinc. World Health Organization data demonstrates that administering 20 milligrams of zinc daily for 10 to 14 days drastically reduces the duration of acute stool frequency by 25 percent. It also prevents subsequent episodes for the following three months.
How Zinc Rebuilds the Intestinal Wall
The cellular architecture of your gut gets absolutely pulverized during a severe diarrheal bout. Zinc acts as a microscopic construction crew, accelerating epithelial cell regeneration and boosting local enzyme production. It modifies the tight junctions between your intestinal cells, effectively sealing the leaks that let fluid pour out. But do not expect a standard salt solution to provide this element. You need targeted supplementation alongside your standard electrolyte fluids to truly fortify the mucosal barrier against invading pathogens.
Frequently Asked Questions
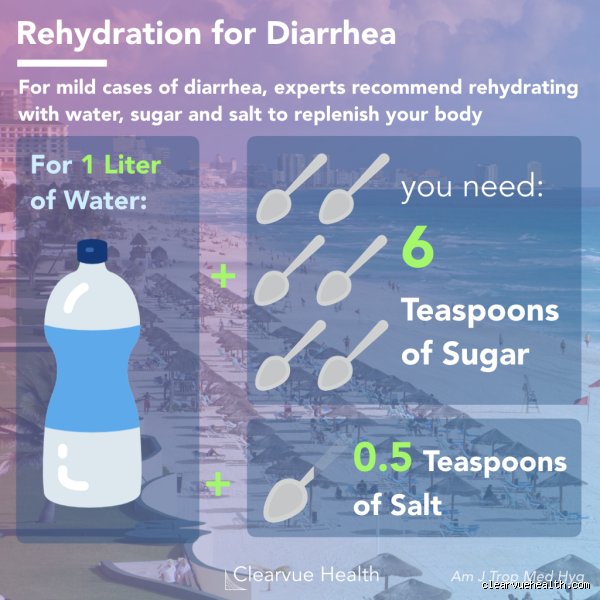
Does salt water stop diarrhea if you add white sugar?
Plain saline solutions lack the necessary mechanism to facilitate rapid hydration, but adding glucose transforms the entire process. The human body utilizes a specific transport protein called SGLT1, which requires exactly two molecules of sodium to escort one molecule of glucose across the intestinal wall. Clinical data confirms that an ideal formulation consists of 2.6 grams of salt and 13.5 grams of anhydrous glucose dissolved in one liter of clean water. This specific combination exploits the sodium-glucose cotransport system, which coaxes the bowel into absorbing water even when it is severely inflamed. In short, adding the correct ratio of sugar is mandatory for the salt to have any anti-diarrheal efficacy at all.
Can coconut water be used as a substitute for standard rehydration solutions?
Coconut water possesses an excellent reputation among fitness enthusiasts, but its specific biochemical profile is suboptimal for severe fluid loss. It contains high levels of potassium yet lacks the necessary concentration of sodium required to correct severe extracellular fluid depletion. A standard clinical diarrheal episode depletes sodium far more aggressively than potassium, meaning coconut water alone cannot restore the necessary systemic equilibrium. You would need to add a pinch of table salt to the coconut fluid to make it a viable substitute during a gastrointestinal crisis. Which explains why relying solely on unadulterated coconut water can leave an individual dangerously hyponatremic during prolonged illnesses.
How long should you wait before seeking professional medical attention?
An adult can typically manage mild symptoms at home for roughly 48 hours using properly balanced oral rehydration formulas. However, the issue remains that certain red flag symptoms demand immediate clinical intervention rather than home-brewed remedies. If you experience a high fever exceeding 102 degrees Fahrenheit, severe abdominal pain, or stools that appear black or contains visible blood, you must visit an emergency room. Infants and elderly individuals possess a much smaller physiological margin for error and can succumb to hypovolemic shock within a mere 24 hours. Never let internet advice replace a professional medical diagnosis when systemic dehydration begins causing dizziness or extreme lethargy.
An Uncompromising Look at Gastrointestinal Recovery
Stop looking for a magical kitchen cure because a simple glass of salty water is never going to fix a raging viral or bacterial infection. We must abandon archaic home remedies that rely on pure guesswork and instead embrace standard, scientifically validated oral rehydration salts. The physiological reality is harsh: your intestines do not care about internet folklore, they care about precise osmolarity. Dehydration kills over 500,000 children globally every single year, a tragic statistic that highlights the absolute necessity of proper clinical protocols. Treat your body like a complex biological machine, not a laboratory for unmeasured kitchen experiments. Invest in genuine rehydration packets, monitor your fluid output meticulously, and consult a doctor the moment your symptoms spiral out of control.