Decoding the latest epidemiological data on autism spectrum disorder
The dramatic reversal of historical diagnostic trends
For twenty years, the prevailing wisdom insisted that white kids were somehow more prone to neurodevelopmental conditions. Honestly, it's unclear how that myth survived so long under serious scrutiny. The reality is that the Autism and Developmental Disabilities Monitoring Network, which has been tracking these metrics since 2000, recently revealed a massive flip. In their exhaustive 2025 community report, researchers analyzed the health and special education records of thousands of eight-year-olds across 16 distinct surveillance sites. What they uncovered shocked the traditionalists. White children now sit at the bottom of the prevalence ladder, coming in at 27.7 per 1,000 children. That changes everything we thought we knew about the distribution of neurodiversity.
A closer look at the peak figures
Where it gets tricky is looking at the top of that specific ladder. Asian or Pacific Islander children recorded a prevalence rate of 38.2 per 1,000 children, while American Indian or Alaska Native communities registered at 37.5 per 1,000. Black children were not far behind at 36.6 per 1,000. People don't think about this enough, but those gaps represent thousands of real families navigating complex school systems and clinical evaluations. The data points to a massive, systemic reorganization of how we identify behavioral traits in different neighborhoods, shifting the needle toward minority groups who were previously left in the dark.
Why the shift in autism identification rates is happening now
The erosion of systemic and economic barriers
We are witnessing the belated fruits of targeted public health campaigns. Historically, getting an official diagnosis required money, time, and a pediatrician who actually listened to your concerns. If you lived in an underfunded ZIP code, your kid wasn't labeled autistic; they were just labeled problematic. But the thing is, decades of advocacy by organizations like the Autism Society of America finally cracked open the door to early screening toolkits in urban clinics and community centers. Medicaid expansions and mandated school screenings chipped away at the wall that kept minority children out of the data pool. The issue remains, however, whether this surge is a true biological representation or a frantic catching-up period for communities that were structurally ignored for generations.
The role of clinical bias and changing criteria
Clinicians are human, which means they carry baggage. For years, a wealthy white boy lining up toy trains was the textbook archetype of autism spectrum disorder. But what happens when a Black child presents with the exact same repetitive behaviors? Too often, they were funneled into oppositional defiant disorder pipelines instead of receiving supportive neurodevelopmental therapies. As diagnostic criteria in the DSM-5 shifted to place greater emphasis on sensory processing and a broader spectrum of social communication deficits, the old gatekeeping mechanisms began to fail. And as clinicians became better trained to look past their own cultural blind spots, the numbers adjusted accordingly.
Investigating the co-occurrence of intellectual disabilities across racial groups
The troubling disparity in diagnostic severity
This is where the story takes a dark turn, and it is precisely where my own view hardens against the celebratory narrative of "better tracking." It is easy to look at rising numbers and celebrate progress, except that the underlying details show a persistent, ugly inequity. When you look at the children diagnosed with autism spectrum disorder, the percentage who also have a documented intellectual disability varies wildly by race. Among Black children identified with autism, a staggering 52.8% also possess an intellectual disability. Compare that to just 32.7% of white children. Why such a massive gulf? The answer isn't genetic vulnerability.
Late detection and missed opportunities
The stark difference in intellectual disability rates suggests that minority children are still only being caught by the system when their support needs are incredibly high. A white child with average or high intelligence who struggles socially might get a gentle, early diagnosis at age three because their parents have the leverage to demand a specialist. But a Hispanic or Black child with the same profile is frequently missed entirely until they face severe academic failure or behavioral crises later in elementary school. As a result: by the time the state finally records them in an official database, their challenges have compounded. We aren't necessarily seeing a higher natural rate of autism in minority populations; we might just be seeing the wreckage of delayed intervention.
How geography and local infrastructure distort national statistics
The California anomaly versus the rest of the nation
To truly understand how unreliable raw national numbers can be, you have to look at the wild geographic swings within the federal tracking network itself. In California, where state-funded regional centers provide a robust, legally mandated safety net for developmental services, the recorded autism rate soared to 1 in 19 children. Now look at Laredo, Texas, where the infrastructure is practically non-existent by comparison. There, the recorded rate plummets to 1 in 103. Did a mystical wind blow across the state line to alter the neurology of children born in the Southwest? Obviously not. The contrast proves that local policy, wealth, and school funding dictate the numbers far more than any innate racial characteristic ever could.
The danger of drawing definitive biological conclusions
Drawing sweeping conclusions about racial genetics based on these public health reports is an exercise in statistical illiteracy. When we say one group has the highest rate, we are actually saying that group has the highest rate of *detected* cases within a highly flawed, fragmented American medical system. Some academic experts disagree on the exact margins, but almost everyone agrees that environmental, economic, and systemic factors form a tangled web that is currently impossible to unknot. In short, the numbers tell us a great deal about the behavior of our institutions, but they tell us very little about the immutable nature of race.
Common mistakes and widespread misconceptions
The illusion of genetic destiny
We often fall into the trap of assuming that because autism is highly heritable, racial disparities in prevalence maps must reflect pure genetic divergence. The problem is that genes do not operate in a vacuum. When data shows certain groups tracking higher numbers, observers instantly leap to biological determinism, ignoring how systemic screening mechanisms actually operate. Let's be clear: a DNA sequence does not dictate administrative visibility. Wealthy school districts possess the resources to flag neurodivergence early, which explains why affluent enclaves often show inflated diagnostic tallies compared to marginalized neighborhoods. We confuse a clinical paper trail with biological reality, rendering our understanding of what race has the highest autism rate fundamentally skewed by postal codes.
The universal diagnostic checklist fallacy
Diagnostic criteria were originally calibrated using a highly specific, narrow cohort of white, middle-class males. Because behavior is filtered through cultural lenses, manifestations of neurodivergence are routinely misread by educators and clinicians alike. Black and Hispanic children exhibiting repetitive behaviors or social communication differences are frequently tracked into behavioral modification pipelines or misdiagnosed with oppositional defiant disorder instead of receiving an accurate developmental evaluation. It is an exercise in systemic irony that the exact same behavioral presentation yields a therapeutic support plan for one child and a disciplinary referral for another. But parsing these nuances requires looking past raw spreadsheets to see the underlying structural biases.
The hidden paradigm: Diagnostic migration and administrative camouflage
How shifting categories mask the true data
An overlooked dimension in evaluating which demographic groups experience higher diagnostic frequencies is the phenomenon of diagnostic migration. In historical datasets, Black children were disproportionately labeled with intellectual disabilities rather than autism spectrum conditions. As clinical awareness shifted, these administrative labels evolved, causing an apparent explosion in autism numbers within specific communities without any actual change in the underlying population trait. The issue remains that historical tracking was profoundly flawed, making contemporary longitudinal comparisons incredibly deceptive. If you look closely at the CDC’s Autism and Developmental Disabilities Monitoring Network data, the recent equalization of prevalence rates across racial groups is less about biology shifting and more about minority communities finally catching up to the baseline of clinical access.
Frequently Asked Questions
Which demographic group shows the highest documented prevalence in recent United States surveillance?
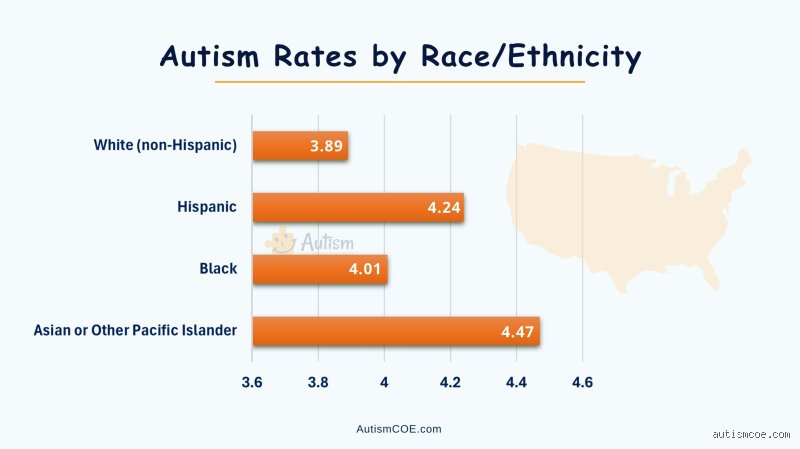
According to the most recent comprehensive surveillance reports published by the Centers for Disease Control and Prevention tracking 8-year-old children, prevalence of autism spectrum disorder reached approximately 1 in 36 children overall. When broken down by demographic categories, the data revealed that prevalence estimates were notably higher among Black, Hispanic, and Asian or Pacific Islander children compared to White children. Specifically, the identified prevalence hovered around 3.3% for Black children and 3.2% for Hispanic youth, whereas the documented rate for White children sat at approximately 2.4%. This inversion of historical trends marks the first time since tracking began that minority groups have outpaced white cohorts in administrative records, reflecting a massive surge in targeted community screening initiatives rather than a sudden shift in genetic distribution.
Why did older medical studies consistently report that white children had the highest autism rate?
For decades, epidemiological data suffered from severe ascertainment bias because clinical infrastructure was heavily concentrated in affluent, predominantly white suburban areas. Families with significant financial means and health literacy could navigate complex diagnostic matrices, secure private evaluations, and demand school accommodations, which naturally created an artificial statistical mountain. As a result: early medical literature mistakenly concluded that Caucasian ancestry carried an inherent vulnerability to the condition. Lower-income families and families of color faced systemic barriers including language obstacles, lack of insurance coverage, and a scarcity of specialized pediatricians, ensuring their children remained invisible to state and federal surveillance registries until adulthood. Are we really supposed to believe the biology changed overnight simply because the diagnostic clinics finally opened their doors in urban centers?
Can socioeconomic status completely account for the differences we see in racial autism data?
Socioeconomic status explains a massive portion of the statistical variance, yet it cannot completely account for the entire discrepancy due to the intersecting nature of healthcare biases. Even when controlling for income levels, families of color frequently experience longer wait times between their initial parental concern and the formal confirmation of a diagnosis. Maternal health disparities, prenatal exposure to environmental toxins in industrialized zones, and differing levels of trust in institutional medicine also influence who gets tracked into the system and who slips through the cracks entirely. In short, wealth provides a buffer that amplifies diagnostic visibility, but cultural stigma within specific communities and institutional racism within the medical establishment continue to warp the data independently of a family's bank account balance.
A definitive perspective on neurodevelopmental tracking
Obsessing over the question of what race has the highest autism rate is entirely missing the point of modern epidemiology (and wasting precious clinical resources in the process). The numbers we obsess over do not reflect fixed biological realities; they mirror our societal willingness to screen, validate, and support vulnerable children. We must recognize that the recent statistical surge in minority communities represents a triumph of public health outreach rather than an epidemic of pathology. Equity is not achieved when numbers match perfectly on a spreadsheet, but when access to early intervention is decoupled from race and class entirely. Let's stop treating these shifting percentages as a genetic race and start viewing them as a diagnostic report card on our healthcare system's deep-seated inequities.