The Evolution of Neurodiversity Across Demographics
For decades, the standard archetype of an autistic child was a wealthy, White male who had access to elite clinical specialists. This skewed the baseline data. The apparent explosion in minority diagnoses isn't a sudden biological surge, because autism does not care about skin color. It is an artifact of better screening. When the Autism and Developmental Disabilities Monitoring (ADDM) Network started tracking these numbers in 2000, White children were consistently identified at much higher rates than their peers.
Shifting Baselines in Early Intervention
What changed? Public health initiatives in states like California and New York deliberately targeted underserved communities, forcing pediatrician offices to implement universal screening tools at 18 and 24 months. Because of this, kids who would have previously been labeled as "difficult" or "speech-delayed" are now getting the correct neurodevelopmental paperwork. It is a massive bureaucratic correction. Yet, the question lingers: are we seeing the true ceiling of these numbers, or is this just the tip of an iceberg?
The Complexities of Diagnostic Criteria
Where it gets tricky is how the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) is applied in different cultural contexts. Behavior that looks like a core symptom of Autism Spectrum Disorder (ASD)—such as poor eye contact—might actually be a sign of respect in certain Asian or Native American households, which explains why Asian prevalence rates often fluctuate wildly depending on the specific state database you examine. Clinicians are human. They bring their own cultural baggage to the evaluation table, sometimes misinterpreting cultural nuances as developmental deficits or vice versa.
Decoding the 2023 and 2026 CDC Surveillance Data
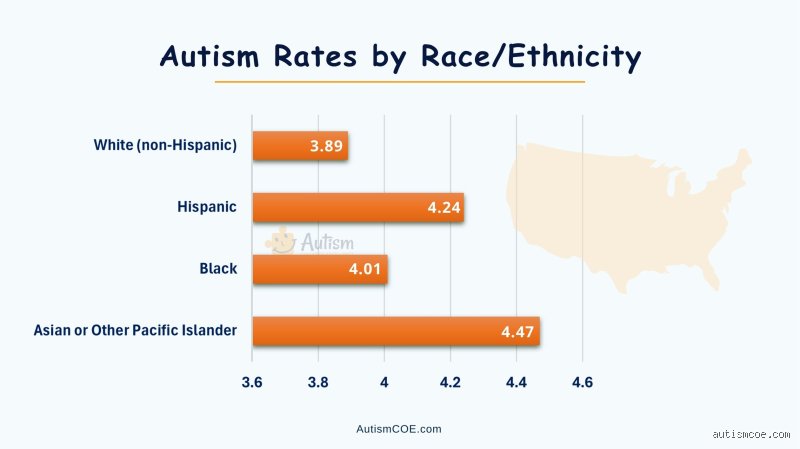
If we look closely at the numbers released by the ADDM Network, the stats tell a jarring story about American healthcare. In the 2023 report cycle, which analyzed data from 11 distinct communities across the country, one in 36 children met the criteria for ASD. But when you disaggregate that massive dataset by race, the old narrative shatters completely. Black children were identified at a rate of 29.3 per 1,000, Hispanic children at 27.3 per 1,000, and White children at 24.3 per 1,000.
People don't think about this enough. Why did White families suddenly drop to the bottom of the statistical ladder in major metropolitan areas? Well, the issue remains that affluent demographics often bypass public school evaluations entirely. They seek private, out-of-pocket neuropsychological assessments that do not always get funneled into state-funded public health databases, which means the official numbers might actually undercount wealthy White children while overrepresenting communities that rely strictly on Medicaid-funded school interventions.
The Socioeconomic Catalyst in Medicaid States
Consider Minnesota. In Minneapolis, researchers found that Somali immigrant communities showed remarkably high rates of autism with profound intellectual impairment, a phenomenon that triggered intense scientific scrutiny and a bit of local panic. Was it environmental? Was it genetic? Honestly, it's unclear, except that subsequent investigations pointed heavily toward heightened parental awareness and intensive local screening efforts targeting that specific diaspora. That changes everything because it proves that prevalence is directly proportional to how hard a society is looking for it.
The Paradox of Higher Identification Rates
But wait, does a higher diagnosis rate mean better outcomes? We are far from it. I believe we are witnessing a hollow victory where minority children are labeled faster but still wait months—sometimes years—for actual behavioral therapies due to systemic underfunding in urban school districts. A diagnosis on a piece of paper is useless without the funding to back it up.
Cultural Barriers and the Invisible Spectrum
Stigma is a brutal filter. In many first-generation immigrant households, admitting a child has a neurological difference is viewed as a profound family failure or a spiritual curse, hence the severe underreporting in certain Asian-American subgroups where numbers remain lower than the national average. A child might mask their repetitive behaviors or repetitive speech patterns perfectly at home, only to melt down in the chaotic environment of an American public school classroom.
The Language Barrier in Clinical Settings
Imagine trying to explain the nuanced difference between a tantrum and a sensory meltdown when English is your third language. Interpreters in medical clinics often lack the specialized vocabulary to translate terms like "stimming" or "joint attention" accurately, as a result: parents leave the clinic with a generic global developmental delay diagnosis instead of the specific autism classification needed to unlock specialized state funding. It is a logistical nightmare that locks thousands of families out of the system entirely.
Comparing Global Prevalence: The Western Bias
When you step outside the American bubble, the global data becomes even more chaotic and fragmented. The United Kingdom's National Health Service (NHS) reports similar trends, with Black Caribbean children showing higher rates of identified autism compared to their White British peers, a reality driven by similar urban screening dynamics. But if you look at South Korea, a landmark study led by Dr. Young-Shin Kim revealed a staggering prevalence of 2.64% in a general population school sample—most of whom were completely undiagnosed before the researchers arrived. Why? Because the school system there simply absorbed these quirky, hyper-focused students without formally labeling them.
The Problem with Universal Checklists
We rely on diagnostic tools developed almost exclusively in Western universities using white, middle-class test subjects. Can a screening tool designed in London or Boston truly measure neurodivergence in a child growing up in rural Peru or Tokyo? The short answer is no, because the behavioral benchmarks themselves are deeply rooted in Western cultural expectations of independence and social interaction. Until we create culturally agnostic diagnostic criteria, trying to declare which ethnicity has the most autism is a fool's errand. We are merely measuring who has the most aggressive diagnostic infrastructure.
Common Mistakes and Misconceptions in Autism Demographics
The Illusion of the "White Boy" Phenomenon
For decades, clinicians operated under the delusion that autism spectrum disorder exclusively selected affluent white males. It was a textbook case of selection bias. White, upper-middle-class families possessed the capital to navigate labyrinthine medical systems, leaving minority communities entirely in the dark. Let's be clear: autism prevalence disparities are largely administrative artifacts, not biological truths. When you look at historical diagnostic rates, you are not viewing the genetic reality of what ethnicity has the most autism; you are looking at an architectural map of healthcare privilege. The issue remains that historical screening tools were calibrated using data from homogeneous, white cohorts, rendering them blunt instruments when applied to diverse populations.
Confusing Diagnostic Surge with Biological Increase
Because the Centers for Disease Control and Prevention (CDC) reported in recent Autism and Developmental Disabilities Monitoring (ADDM) network cycles that Black and Hispanic children are now identified at higher rates than white children, commentators panicked. They assumed a biological shift had occurred. Except that this surge merely reflects narrowed gaps in screening efficacy. In 2020, ADDM data showed autism prevalence reached 2.8% in Black, Hispanic, and Asian children compared to 2.4% in white children. Does this answer what race has the highest rate of autism definitively? No. It proves that targeted community outreach finally started working, catching cases that previously evaporated into school disciplinary statistics or incorrect intellectual disability diagnoses.
The Hidden Reality of Diagnostic Migrations
How Minority Families Navigate Clinical Erasure
Medical gaslighting takes a specific, insidious form when race intersects with neurodivergence. Black children exhibiting identical autistic traits to their white peers are frequently misdiagnosed with Oppositional Defiant Disorder (ODD) or conduct conditions. Why does this happen? The problem is an ingrained cultural myopia within the psychiatric establishment. And it carries devastating real-world consequences, channeling children into the carceral state rather than therapeutic environments. (Think about the sheer cognitive dissonance required to label a non-verbal child's meltdown as malicious rebellion.) As a result: ethnic minority autism statistics remain artificially suppressed in older cohorts because these individuals were funneled into entirely different diagnostic categories during their formative years.
The Linguistic Barrier to Accurate Prevalence Tracking
Consider the logistical nightmare facing a non-English speaking immigrant family navigating a Western developmental evaluation. Standardized diagnostic instruments, like the Autism Diagnostic Observation Schedule (ADOS), do not translate seamlessly across cultural contexts. Subtle nuances of eye contact, joint attention, and social reciprocity are deeply bound by cultural norms. An evaluator might misinterpret a Hispanic child's respectful deferential gaze as an autistic deficit in social communication, or conversely, miss restrictive behaviors due to language barriers. True diagnostic equity cannot exist until evaluation tools are completely decoupled from Eurocentric behavioral benchmarks.
Frequently Asked Questions
Which ethnic group is diagnosed with autism most frequently in the United States?
Recent epidemiological tracking indicates that Hispanic and Black children currently exhibit the highest identified prevalence of autism spectrum disorder in the United States. According to the CDC's 2023 surveillance summary, which analyzed 8-year-old children across 11 regional sites, prevalence estimated that 1 in 36 children had an autism spectrum disorder diagnosis, with rates among Black (2.9%) and Hispanic (3.2%) youth slightly outpacing white cohorts (2.4%). This represents a massive historical inversion from two decades prior, when white children were diagnosed at significantly higher frequencies. The shift is universally attributed to intensive community screening initiatives and expanded Medicaid coverage, rather than a sudden shift in population genetics. Consequently, the data reveals which ethnic group has the highest rate of autism purely through the lens of modern clinical identification success.
Are there global genetic differences in autism rates across different races?
Global epidemiological data indicates that genomic vulnerabilities to autism spectrum disorder remain remarkably stable across all human populations, meaning no single race possesses an intrinsic genetic predisposition to the condition. While localized studies in places like Sweden report a 1.5% prevalence and parts of Asia, particularly South Korea, have yielded figures as high as 2.64%, these variances reflect diagnostic thresholds and study methodologies rather than distinct genetic architecture. Human genetic variation is vastly greater within any single ethnic population than it is between different racial groups. Phenotypic expression of autism varies globally based on environmental triggers, maternal health access, and toxicant exposures, but the underlying neurodevelopmental variations do not favor any specific continent. In short, looking for a biological epicenter for neurodivergence across racial lines is a scientifically bankrupt endeavor.
How does socioeconomic status affect autism diagnosis across ethnicities?
Socioeconomic status acts as a ruthless filter that distorts our understanding of what ethnicity has the most autism by controlling who gains entry into the clinical pipeline. Wealthier families can bypass multi-year public waiting lists by paying for private neuropsychological evaluations, which can easily cost upward of $5,000. This financial leverage grants them earlier access to intensive behavioral interventions and specialized educational accommodations. Meanwhile, lower-income minority families rely on underfunded school districts to spot developmental delays, which explains why their children are often diagnosed much later in life, if at all. This economic disparity creates a skewed data pool where affluent white children receive nuanced neurodevelopmental profiles, while impoverished minority children are left invisible to state registries.
A Radical Shift in the Neurodiversity Paradigm
We must abandon the archaic obsession with ranking human populations by diagnostic density. Obsessing over what race has the most autism distracts us from the systemic failures occurring at the intersection of race, poverty, and medicine. The data tells us that when you level the socio-economic playing field, neurodivergence shows no racial favoritism. It is time to stop viewing autism as a white, suburban monoculture and start funding culturally competent diagnostic infrastructure. We need to actively reallocate resources to underserved communities instead of merely observing their rising statistics from afar. True medical progress is not measured by how neatly we categorize human variance, but by how effectively we support the vulnerable across every demographic border.