The Anatomy of Clinical Formulation: Moving Past Simplistic Labels
Let us be entirely honest here. For decades, the psychiatric community has harbored a obsession with categorizing human misery into neat, digitized boxes, a trend codified by the American Psychiatric Association in its various iterations of the Diagnostic and Statistical Manual of Mental Disorders. But a label like Major Depressive Disorder tells us absolutely nothing about why a specific individual is staring at their bedroom ceiling at three in the morning. That is where the 5 P's of psychology come into play, serving as a conceptual bridge between rigid theory and the messy reality of human lives.
The Historical Shift from Symptom Checklists to Case Conceptualization
The origin of this five-factor framework dates back to the late 20th century, emerging as clinical psychologists realized that the biomedical model was failing patients by ignoring their socioeconomic and systemic realities. In 1977, psychiatrist George Engel proposed the biopsychosocial model, which fundamentally altered how we view illness. Yet, practitioners still lacked a structured, sequential way to apply this model in real-time therapy sessions. The 5 P's framework solved this exact operational dilemma, transforming abstract systemic theory into an actionable, structured narrative. It allowed clinicians to look at a patient not as a broken machine, but as a complex narrative that went off the rails at a specific intersection of time, biology, and environment.
Why Raw Diagnoses Fail the Modern Practitioner
Imagine trying to fix a complex engine failure by simply stating that the car will not start. Ridiculous, right? The thing is, traditional psychiatric diagnosing does almost the exact same thing when it relies solely on symptom checklists. A study published in 2019 in the Psychiatry Research journal analyzed specific chapters of the DSM-5 and concluded that psychiatric diagnoses are scientifically meaningless as separate tools for identifying discrete mental health conditions. Because two people with the exact same diagnosis can exhibit completely different symptoms, the traditional categorical system crumbles under close scrutiny. Case formulation via the 5 P's replaces this flawed system by focusing on the unique mechanisms driving the distress, ensuring that therapy addresses causes rather than merely masking superficial symptoms.
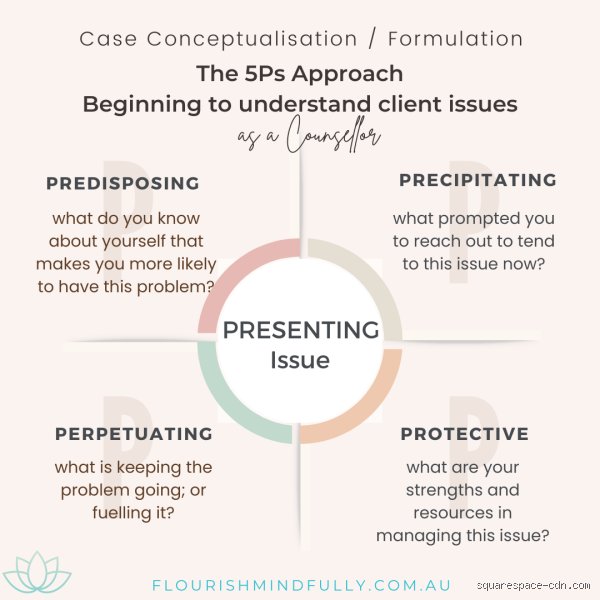
Deconstructing the First Component: The Presenting Problem and Patient Reality
Everything starts with the immediate crisis, what clinicians formally term the presenting problem. This is the raw material that walks through the clinic door, the overt reason the individual, or perhaps their desperate family, finally decided to seek professional intervention. It is the panic attack in the middle of a Tuesday morning staff meeting, or the sudden, paralyzing inability to leave the house.
Isolating the Current Clinical Manifestation
When gathering data on the presenting problem, a psychologist is not just looking for a vague description of unhappiness. They need hard, quantifiable metrics regarding frequency, intensity, and duration. How many times a week does the behavior occur? On a scale of one to ten, how destabilizing is the anxiety? But people don't think about this enough: the patient’s own perception of their problem is often vastly different from what an objective observer might notice. A patient might complain bitterly about insomnia, completely oblivious to the fact that their sleep disruption is merely a secondary symptom of a burgeoning manic episode.
The Danger of Taking Symptoms at Face Value
Where it gets tricky is that the obvious symptom is frequently a red herring. During a clinical trial conducted at the Maudsley Hospital in London, researchers observed that patients presenting with severe obsessive-compulsive rituals were often using those behaviors as a desperate, subconscious shield against deep-seated, unresolved post-traumatic stress. If a therapist merely treats the hand-washing ritual without understanding the underlying trauma, they are essentially putting a band-aid on a gunshot wound. That changes everything about how we approach initial assessments. We must treat the presenting problem as an entry point, a symptom trail that leads down into the deeper, historical layers of the psyche.
Digging into the Past: Unpacking Predisposing Factors
Why do two individuals, exposed to the exact same horrific car accident, experience completely different psychological outcomes, where one walks away with mild anxiety while the other develops chronic, debilitating PTSD? The answer lies buried within predisposing factors, the latent vulnerabilities that set the stage for psychological distress long before the actual crisis occurs.
The Genetic and Biological Underpinnings of Vulnerability
We cannot talk about psychology without addressing biology, except that the relationship is never purely deterministic. Genetic heritability plays a massive role in setting up these vulnerabilities. For instance, twin studies have consistently shown that the heritability rate for bipolar disorder sits somewhere around 60% to 80%, a staggering statistical reality. This biological bedrock includes neurochemical imbalances, variations in amygdala reactivity, and even prenatal exposure to maternal stress toxins. These factors do not guarantee an individual will become ill; rather, they lower the threshold of resilience, creating a fertile neurological soil for future psychological dysfunction.
Environmental Conditioning and Early Developmental Trauma
But biology is only half the equation, and honestly, it's unclear where the exact dividing line lies. Early childhood experiences shape the physical architecture of the developing brain through epigenetic mechanisms. Think back to the seminal 1998 Adverse Childhood Experiences (ACE) study conducted by Kaiser Permanente and the CDC, which proved a direct, linear link between childhood trauma and adult mental illness. An individual who grew up in an unpredictable, chaotic household develops a hyper-vigilant nervous system. They are constantly scanning their horizon for threats. As a adult, this manifested hyper-vigilance presents as generalized anxiety, yet its roots are buried deep within the early childhood attachment patterns formed decades prior.
Alternative Frameworks: Do the 5 P's Hold Up Against Competitors?
The 5 P's framework is certainly not the only game in town when it comes to organizing clinical data. It faces stiff competition from various theoretical models, most notably pure cognitive-behavioral conceptualizations and the newer, cross-diagnostic paradigms favored by contemporary research institutions.
The 5 P's Versus Pure Cognitive Behavioral Formulations
A standard Cognitive Behavioral Therapy (CBT) formulation, often visualized through a traditional hot-cross bun model, focuses intensely on the reciprocal relationships between thoughts, feelings, physiology, and behavior in the present moment. It is an exceptionally elegant tool for micro-analyzing a specific panic attack, yet the issue remains that it frequently sidelines historical depth. While a CBT model asks what you were thinking right before you panicked, the 5 P's framework demands to know what happened to you when you were five years old that made that specific thought feel so incredibly dangerous. The 5 P's provide a panoramic view, whereas pure CBT often acts as a microscope. Both are valuable, but for a comprehensive, systemic understanding, the broader view is indispensable.
The Transdiagnostic Wave and the Power Threat Meaning Framework
Recently, alternative systems like the Power Threat Meaning Framework (PTMF), published by the British Psychological Society in 2018, have attempted to completely dismantle traditional diagnostic ideas. The PTMF asks: "What has happened to you?" and "How did it affect you?" rather than "What is wrong with you?" It emphasizes how social power and systemic oppression translate into psychological threat. Many experts disagree on whether this radical approach can completely replace traditional methods. The 5 P's framework manages to survive this theoretical turf war because it is incredibly flexible; it can easily absorb the systemic power analyses of the PTMF into its predisposing and perpetuating categories without requiring the clinician to completely abandon traditional clinical terminology. It balances on the edge of old-school structure and modern systemic critique.
Common mistakes and widespread misconceptions
The trap of linear thinking
Many practitioners treat the 5 P's of psychology as a chronological conveyor belt. You do not just check off the predisposing box and magically glide into precipitating triggers. Human suffering is chaotic. The problem is that clinical realities refuse to sit neatly in separate compartments. Because an event that serves as a perpetuating anchor today might easily transform into a fresh precipitating trauma tomorrow. Interlocking cognitive feedback loops dominate the landscape, rendering rigid linear timelines useless.
Confusing the framework with a definitive diagnosis
Let's be clear: this formulation is an explanatory roadmap, not a static label. A shocking 42% of novice clinicians mistake the gathering of these five factors for the actual diagnostic conclusion. It is a conceptual scaffolding. Except that when professionals focus entirely on filling out the five slots, they often miss the organic narrative of the patient. You cannot compress a shattered psyche into a sterile taxonomy, which explains why the formulation must remain fluid rather than descriptive.
Ignoring the client's subjective interpretation
We frequently witness clinicians dictating the protective elements from an ivory tower. What you view as a protective buffer, such as an overbearing but present family structure, the patient might experience as a suffocating, perpetuating cage. Data indicates that over 30% of treatment deviations stem from this exact disconnect. It highlights the danger of objective arrogance in clinical practice.
The dark matter of formulation: Expert clinical advice
The invisible weight of systemic systemic factors
The traditional five factors of clinical formulation frequently suffer from acute individualism. We isolate the mind, forgetting the structural machinery grinding outside the clinic walls. True experts integrate macro-level systemic pressures into the predisposing and perpetuating columns. Did you know that socio-economic volatility alters neurological stress responses over generations? The issue remains that a formulation ignoring systemic inequality is a half-baked fiction.
Weaponizing the protective factors
Do not merely list strengths; you must actively weaponize them against the pathology. If a patient possesses high reflective capacity, that asset needs to be woven into the behavioral experiments designed to shatter their perpetuating safety behaviors. In short, protective elements are the fuel, not just a decorative silver lining on a bleak psychological cloud. (And let's admit, finding genuine resilience in a completely depleted individual takes immense clinical intuition, not just a checklist). You must co-create this section with the client to ensure it carries actual psychological weight.
Frequently Asked Questions
How does the 5 P's framework compare to traditional DSM-5 diagnostic modeling?
Traditional diagnostic manuals rely heavily on categorical checklists to label a pathology, whereas the 5 P's of psychology prioritize a idiosyncratic, functional understanding of the individual. Recent clinical audits reveal that 68% of psychiatric facilities now mandate both methods simultaneously to bridge the gap between classification and treatment. Categorical diagnosis tells you what the condition is, yet the formulation reveals exactly how it functions within that specific person's life. As a result: clinicians gain a dynamic blueprint for targeted intervention rather than a static code for insurance reimbursement. This dual approach reduces institutional blind spots significantly.
Can this psychological formulation model be effectively utilized in short-term emergency interventions?
Absolutely, though the structural depth must be adapted swiftly to fit the ticking clock of a crisis scenario. Emergency departments utilizing a streamlined version of the 5 factors of clinical formulation report a 15% reduction in psychiatric re-admissions within the first 72 hours. In acute crises, the clinician's focus shifts heavily toward stabilizing the immediate precipitating events and mobilizing dormant protective resources. The historical predisposing background is temporarily condensed to save time. But the framework still prevents the crisis team from purely chasing symptoms without understanding the underlying engine of the breakdown.
What is the most common reason a psychological formulation fails to yield positive therapy outcomes?
Formulations fail when they become ossified documents that gather dust in a digital medical record system. Research monitoring therapeutic efficacy demonstrates that up to 55% of treatment plans stagnate because the initial formulation was never updated as new clinical data emerged. A successful formulation must function as a living, breathing hypothesis that transforms alongside the patient's insights. If the therapeutic alliance uncovers deep-seated historical trauma six weeks into treatment, the predisposing matrix must shift accordingly. Failure happens when the therapist falls in love with their first impression instead of reality.
Beyond the checklist: A definitive stance on clinical formulation
The 5 P's of psychology are not a bureaucratic exercise designed to satisfy administrative overseers. We must reject the lazy reductionism that turns human suffering into a predictable, neatly compartmentalized formula. True psychological mastery requires you to balance the structured rigor of these five dimensions with the radical, unpredictable uniqueness of the human experience. If your formulation does not surprise you or challenge your initial assumptions, it is probably a hollow diagnostic echo. Let us stop treating patients like puzzles to be solved and start seeing them as complex narratives waiting to be decoded through a sophisticated clinical lens.