The Hidden Mechanics: What Happens Before the Clot Strikes?
Medical textbooks love to paint a neat picture of cardiovascular crises. Yet, the human body rarely plays by the rules, and a pulmonary embolism—frequently abbreviated as PE by clinicians in emergency departments from Boston to Berlin—is notoriously chaotic. At its core, this condition occurs when a thrombus, typically a deep vein thrombosis formed in the deep venous system of the lower extremities, detaches itself from the vessel wall. It travels through the inferior vena cava, passes through the right atrium and ventricle of the heart, and forcefully wedges itself into the pulmonary arterial bed.
The Myth of the Dramatic Collapse
People don't think about this enough: a blockage doesn't always announce itself with a Hollywood-style collapse. Honestly, it's unclear why some individuals maintain relatively stable oxygen saturation levels even with a significant submassive clot, while others experience immediate hemodynamic instability from a much smaller obstruction. I am convinced that our collective obsession with dramatic, crushing chest pain as the universal sign of a vascular emergency causes thousands of people to dismiss the actual, whispers of a developing crisis. It is a dangerous gamble.
The Virchow Triad Connection
To understand the timeline, we have to look at what Dr. Rudolf Virchow identified back in 1856, which clinicians still refer to as Virchow's Triad. This trifecta involves endothelial injury, circulatory stasis, and hypercoagulability. When these three conditions intersect—say, during a 14-hour flight from Singapore to Los Angeles where a passenger remains immobilized—the blood in the deep calf veins begins to pool and thicken. Pulmonary embolism risk factors spiral when these factors combine, turning a simple long-haul trip into a biological setup for a future emergency room visit.
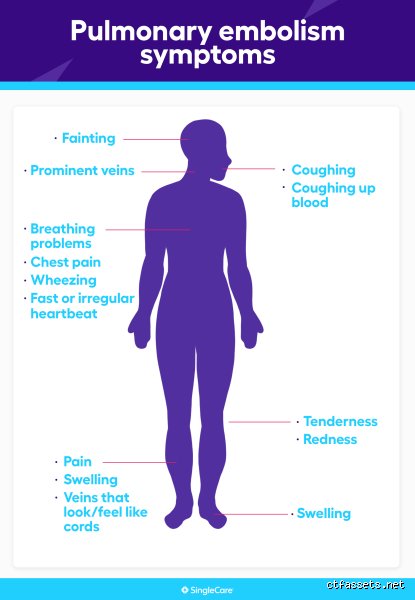
The True Early Warning Signs of a Pulmonary Embolism You Might Dismiss
Where it gets tricky is separating mundane fatigue from a medical emergency. A patient might wake up on a Tuesday morning feeling a bit more winded than usual while walking up a slight incline. Is it just poor cardiovascular conditioning, or is it the first manifestation of a mechanical obstruction in the lungs?
Dyspnea: The Unpredictable Shortness of Breath
Sudden onset dyspnea is the most frequent symptom, appearing in roughly 73% of documented clinical cases. But here is the catch: it can be fleeting. It might hit you while you are washing dishes, lift after five minutes, and then return with a vengeance three hours later when you are merely sitting on the couch watching the evening news. This fluctuating nature often tricks patients into thinking they just swallowed some air wrong or experienced a brief, random spasm of anxiety.
Tachycardia and the Mysterious Racing Pulse
Your heart rate climbs. A normal resting heart rate sits comfortably between 60 and 90 beats per minute, but suddenly your fitness tracker alerts you that your pulse is hovering around 104 while you are doing absolutely nothing. Why does this happen? As the clot obstructs blood flow through the pulmonary artery, the right ventricle must pump significantly harder against this newfound resistance to oxygenate your tissues. As a result: the heart rate accelerates to compensate for the drop in stroke volume, a physiological reflex that can easily be misdiagnosed as sinus tachycardia brought on by too much caffeine or work-related stress.
Pleuritic Chest Pain vs. Muscle Strain
Then comes the pain. Unlike the dull, heavy pressure associated with a myocardial infarction, the discomfort caused by a pulmonary embolism is typically pleuritic. This means it feels sharp, stabbing, and intensely localized, severely worsening every single time you take a deep breath or cough. Except that sometimes it presents merely as a dull ache in the flank or shoulder blade, leading patients to book an appointment with a chiropractor rather than rushing to the nearest level-one trauma center.
The Leg Clot Precursor: Spotting the Origin Point
We cannot talk about the lungs without talking about the legs. Because approximately 70% of PE cases originate from a deep vein thrombosis in the lower thighs or calves, recognizing peripheral vascular symptoms is your absolute best early defense mechanism.
Unilateral Swelling and the Homan's Sign Debate
Look at your ankles. Is one significantly larger than the other? If you notice asymmetric edema—where your left calf measures even two centimeters larger in circumference than your right calf—that changes everything. This swelling occurs because the thrombus completely or partially occludes the femoral or popliteal vein, causing venous blood to back up into the surrounding tissue. Did you know that old-school physicians used to rely heavily on Homan's sign, which involves dorsiflexing the foot to see if it elicits pain in the calf? Modern vascular medicine has largely abandoned this test because it is wildly unreliable and, theoretically, could dislodge the clot prematurely, yet the presence of localized warmth and erythema remains a critical diagnostic red flag.
Distinguishing a Pulmonary Embolism from Panic and Asthma
This is where the diagnostic waters get incredibly muddy. The clinical presentation of a pulmonary embolism overlaps almost perfectly with several acute psychiatric and respiratory conditions, creating a dangerous masquerade that puzzles even seasoned triage nurses.
The Panic Attack Trap
Imagine a 28-year-old woman arriving at an urgent care clinic hyperventilating, sweating, and complaining of a racing heart. Given her demographic and lack of prior surgical history, a practitioner might instinctively lean toward a severe panic attack. But what if she started taking an oral contraceptive pill containing desogestrel three months ago? That hormonal shift increases her relative risk of thrombosis by nearly fourfold, meaning that what looks exactly like a mental health crisis could actually be a life-threatening clot. How do you tell them apart when both cause hyperventilation and a sense of impending doom? The issue remains that panic attacks usually subside within thirty minutes, whereas the hypoxia induced by a PE persists regardless of deep breathing exercises or psychological grounding techniques.
Asthma Flare-ups and Chronic Bronchitis
For individuals with a history of reactive airway disease, the diagnostic confusion doubles. An asthma exacerbation involves widespread bronchospasm, typically characterized by diffuse wheezing during expiration. Conversely, a pulmonary embolism rarely causes true wheezing, presenting instead with clear lung sounds upon auscultation or localized rales where the lung tissue is beginning to suffer from localized ischemia. We are far from a world where patient self-diagnosis is safe; relying on your old albuterol inhaler to fix sudden breathlessness could cost you precious time when what your pulmonary vasculature actually needs is an immediate intravenous bolus of unfractionated heparin or a mechanical thrombectomy.
Common Mistakes and Misconceptions Regarding Clot Identification
The Myth of the Mandatory Swollen Leg
Everyone assumes a massive blood clot in the lung starts with a dramatically purple, ballooning calf. The problem is that clinical reality mocks textbook descriptions. Medical literature indicates that roughly 30% of patients with a confirmed pulmonary embolism present with absolutely zero detectable symptoms of deep vein thrombosis in their lower extremities. You might expect excruciating pain while walking, yet your legs look completely pristine. This absence of local swelling tricks individuals into dismissing sudden shortness of breath as mere fatigue. Because the initial clot can completely detach or originate from the pelvic veins, looking for a swollen leg to confirm your suspicion is a dangerous game.
Confusing Acute Respiratory Distress with Panic Attacks
Hyperventilation feels identical to a vascular catastrophe. When a person experiences a sudden spike in heart rate alongside chest tightness, mental health becomes the immediate scapegoat. Except that treating a life-threatening blockage with deep breathing exercises can prove fatal. Clinicians frequently note that young women are disproportionately misdiagnosed with anxiety or panic disorders when experiencing the early warning signs of a pulmonary embolism. If you find yourself gasping for air while sitting perfectly still, do not let anyone convince you it is just stress. Trust your body over a hasty assumption.
Assuming Fitness Grants Total Immunity
Elite athletes believe their pristine cardiovascular health shields them from vascular events. Let's be clear: extreme physical conditioning can actually mask the subtle physiological shifts that signal an impending crisis. An enlarged right ventricle in an endurance runner might easily tolerate a minor obstruction that would collapse an sedentary individual, hiding the danger until it reaches a critical threshold. Olympians experience trauma, dehydration, and long flights just like everyone else. Your resting heart rate of forty-five beats per minute will not dissolve a fibrin clump once it lodges in your pulmonary arterial bed.
The Hidden Trigger: Micro-Clots and the Post-Infection Window
The Subacute Threat of Viral Insults
We routinely screen orthopedic surgical patients and long-haul travelers for thrombotic risks. But what about the person who recovered from a standard respiratory virus three weeks ago? Recent epidemiological data reveals that the risk of developing a catastrophic lung blockage increases by up to three times normal baseline levels in the thirty days following a severe viral infection. These pathogens trigger a prolonged hypercoagulable state characterized by widespread endothelial inflammation. (This subtle vascular damage remains invisible on routine blood work). Consequently, a person might feel completely recovered from their illness, only to suddenly experience unexplained chest pain while making breakfast.
[Image of pulmonary embolism]Expert Pro-Tip: The Posture Shift Test
How do we differentiate between musculoskeletal strain and a true vascular emergency at home? Pay close attention to how your discomfort responds to gravity. Muscular pleurisy typically alters its intensity when you twist your torso or raise your arms. A clot inside the pulmonary vasculature, however, remains stubbornly indifferent to structural manipulation. The issue remains that the localized ischemic pain from an occluded vessel persists whether you are lying flat, standing up, or hanging upside down. If changing your physical position offers absolutely no relief to that sharp, stabbing sensation in your ribs, your lungs are likely screaming for help.
Frequently Asked Questions
How quickly do the early warning signs of a pulmonary embolism progress?
The temporal evolution of a lung obstruction ranges from a slow, deceptive burn to an instantaneous catastrophic collapse. Data from emergency medicine registries indicates that approximately 10% of acute cases result in sudden death within the first sixty minutes of symptom onset. For the remaining majority, signs like unexplained dyspnea or localized chest discomfort can fluctuate subtly over a window of forty-eight to seventy-two hours before escalating. As a result: waiting to see if your breathing improves overnight represents a massive gamble with your survival. Immediate diagnostic intervention via a computed tomography pulmonary angiography remains the only definitive way to halt this aggressive progression.
Can a standard pulse oximeter detect a pulmonary obstruction early?
Relying solely on a cheap fingertip device to gauge your vascular health provides a dangerously false sense of security. While a plunging oxygen saturation level below 90% certainly signals respiratory distress, early blockages often trigger compensatory hyperventilation that keeps your arterial oxygen levels temporarily normal. Which explains why patients with a significant vascular obstruction can still register a perfect 98% saturation reading during their initial triage. Why gamble your life on a single numerical metric that your body is actively manipulating to survive? True diagnosis requires assessing the ventilation-perfusion mismatch, not just surface oxygenation.
Are certain blood types inherently more susceptible to developing lung clots?
Genetic architecture plays a shockingly quiet yet definitive role in your overall coagulation profile. Large-scale genomic studies confirm that individuals with non-O blood types face a twofold higher risk of suffering from venous thromboembolism compared to those with blood type O. This biological discrepancy stems from elevated baseline levels of von Willebrand factor and factor VIII circulating in AB, A, and B individuals. Yet millions of people remain entirely oblivious to this inherited vulnerability during long-haul travel or hormonal therapies. Knowing your specific blood group should actively dictate your personal level of vigilance regarding unexpected respiratory symptoms.
A Definitive Call to Medical Vigilance
We must dismantle the culture of clinical hesitation that surrounds unexpected respiratory distress. The human body does not generate sudden, inexplicable air hunger without a profound underlying structural failure. Yet we consistently witness patients waiting out their symptoms because they fear embarrassing themselves in an emergency department. In short: discarding your intuition to save face can cost you your life. If you experience an unexplained acceleration of your heart rate combined with a sharp thoracic catch, stop rationalizing the discomfort away. Force the medical establishment to prove you do not have a life-threatening blockage. Your survival depends entirely on demanding aggressive diagnostic clarity before the window of opportunity slams shut forever.