The anatomy of a silent killer: What actually happens before the blockage?
To understand the precursors, we have to look at the plumbing. A pulmonary embolism doesn't just materialize out of thin air in the pulmonary arteries; it almost always begins its journey as a deep vein thrombosis (DVT) in the lower extremities. Imagine a sluggish, stagnant river where debris begins to accumulate against a dam. In the human body, this happens when prolonged immobility, vascular damage, or hypercoagulability causes blood cells to clump together in the deep veins of the calf or thigh. According to data from the Centers for Disease Control and Prevention (CDC), up to 900,000 Americans are affected by DVT or pulmonary embolism each year, yet the public awareness surrounding the initial stages remains shockingly low. Which explains why so many people dismiss the early discomfort as a simple charley horse. I have seen instances where patients spent days massaging a throbbing calf, completely unaware that they were essentially trying to knead an active explosive device deeper into their venous system.
The fatal migration from calf to cardiopulmonary system
Once that thrombus forms, it sits in a state of unstable equilibrium. The issue remains that the clot is structurally fragile. A sudden movement, a change in blood pressure, or even just getting out of bed after a long flight can cause a fragment—or the entire mass—to break away from the vein wall. At this point, it becomes an embolus, riding the fast-moving current of the vena cava straight into the right side of the heart, which then pumps it directly into the pulmonary architecture. When that mass wedges itself into the narrow branches of the pulmonary vasculature, it blocks blood flow, drives up right ventricular pressure, and instantly starves the body of oxygen. This isn't a gradual process; the transition from a localized leg issue to a systemic emergency happens in a heartbeat.
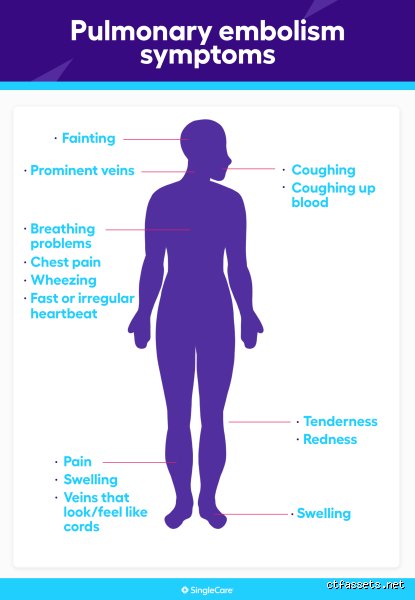
Decoding the deceptive whispers: Early warning signs of a pulmonary embolism
Here is where it gets tricky because the human body is notoriously terrible at pinpointing vascular distress until it is almost too late. Conventional medical wisdom states that you will experience crushing chest pain and sudden gasping, but we're far from it in the days leading up to the event. Instead, the body drops breadcrumbs. The most profound warning sign is an unexplained, persistent elevation in your resting heart rate—a condition known as sinus tachycardia. If your pulse normally hovers around 70 beats per minute but suddenly plateaus at 95 for no discernible reason (even while you are just binge-watching television), your body might be working overtime to pump blood past a developing obstruction. Yet, we rarely check our pulse when we feel slightly off, do we? This subtle autonomic acceleration is frequently accompanied by a fleeting, sharp twinge in the chest that occurs exclusively when taking a deep breath—a classic manifestation of pleuritic friction that people don't think about this enough during its initial presentation.
The unilateral leg swelling paradox
Let us look at the legs, the literal breeding ground for this condition. If you notice that your left ankle looks slightly more puffy than your right, or if your right calf feels unusually warm and sports a faint, dusky reddish discoloration, that changes everything. This asymmetry is the hallmark of an impending crisis. Except that it rarely hurts intensely at first; it feels more like a dull, heavy ache, or a stubborn muscle cramp that refuses to stretch out. Clinical statistics show that roughly 50% of people with a deep vein thrombosis experience no noticeable symptoms at all, making the physical signs that do appear incredibly precious from a diagnostic standpoint. A landmark study published in The Lancet tracked over 10,000 venous thromboembolism patients and revealed that localized unilateral edema was the single most reliable clinical predictor of an underlying clot, outperforming even patient-reported pain scales.
The phantom shortness of breath
Another deceptive precursor is intermittent dyspnea. This isn't the dramatic, suffocating gasping associated with a massive acute blockage, but rather a strange, transient windedness during trivial activities. You walk up a single flight of stairs—a task you have performed daily without a second thought for the last decade—and suddenly you find yourself pausing at the landing, hands on hips, wondering why your lungs feel entirely inadequate. Because the micro-emboli may already be breaking off and showering the lungs, the body is subtly compensating by increasing your respiratory rate. It passes after a minute or two, so you blame aging, or the heavy lunch you just ate, or the humid summer air, but it is actually the prologue to a catastrophic vascular obstruction.
Risk stratification: Who is walking on a diagnostic landmine?
Nobody develops a random blood clot without an underlying trigger, even if that trigger is buried deep within their genetic code. The classic framework for understanding this risk is Virchow's Triad, which isolates three specific pillars: stasis of blood flow, endothelial injury, and hypercoagulability. Honestly, it's unclear why some individuals with multiple risk factors never develop a clot while others with a single, minor vulnerability suffer a massive event; experts disagree on the exact tipping points. But we do know the catalyst variables. Prolonged immobility—such as a non-stop ten-hour flight from Los Angeles to London or a grueling recovery on the couch after orthopedic surgery—creates the perfect environment for blood to pool and solidify in the deep soleal sinuses of the calf.
The compounding effect of modern lifestyles and medications
And then we have the chemical triggers. Estrogen-containing medications, including combined oral contraceptives and hormone replacement therapies, significantly alter the liver's production of clotting factors, tipping the delicate systemic balance toward hypercoagulability. Research indicates that women taking third-generation birth control pills face a three-to-fourfold increase in their risk of developing a venous thromboembolism compared to those who do not. Combine that chemical predisposition with a genetic mutation like Factor V Leiden—a hereditary blood disorders present in roughly 5% of the Caucasian population—and you are suddenly dealing with an exponential amplification of risk. But people rarely get screened for these genetic variants until after they have already survived their first intensive care unit admission.
Differentiating pulmonary embolism warning signs from panic and pneumonia
The diagnostic landscape is cluttered with lookalikes, making early detection a logistical nightmare for patients and triage nurses alike. When you feel a sudden tightness in your chest and your heart begins to race, the immediate psychological response is panic, which, in a cruel twist of biological irony, perfectly mimics the respiratory distress of a pulmonary embolism. As a result: thousands of patients experiencing genuine panic attacks flood emergency departments convinced their lungs are failing, while an equal number of individuals with actual traveling blood clots sit at home, sipping chamomile tea and trying to practice mindfulness. It is a dangerous game of diagnostic roulette where guessing wrong carries a lethal penalty.
The critical diagnostic divergence
| Symptom Profile | Pulmonary Embolism Warning Sign | Panic Attack / Anxiety | Acute Muscle Strain |
| Pain Characteristics | Pleuritic sharp pain that worsens specifically during deep inhalation | Diffuse, crushing tightness centered squarely in the mid-chest area | Localized tenderness that changes when you physically press on the ribs |
| Leg Presentation | Frequent unilateral swelling and warmth in one calf or thigh | No physical changes in the extremities; potential tingling in fingers | Completely absent; pain is strictly confined to the injured muscle zone |
| Onset Trigger | Spontaneous, often following periods of prolonged stasis or surgery | Frequently linked to psychological stressors or sudden emotional triggers | Directly follows mechanical exertion, lifting, or sudden twisting motions |
Look closely at how the pain behaves when you alter your physical positioning. If you pull a chest muscle while lifting weights at the gym, the resulting discomfort will typically flare up when you twist your torso or press your fingers directly onto the intercostal spaces. A pulmonary clot doesn't care if you press on your chest; the pain is internal, visceral, and tied entirely to the mechanical movement of your pleura rubbing against inflamed lung tissue. In short, if the pain stays identical when you change positions but spikes sharply the moment you try to take a maximal breath, you are likely looking at a vascular event rather than a musculoskeletal mishap.
Common mistakes and dangerous misconceptions
The "Hollywood cardiac" illusion
We all know the cinematic trope. A character clutches their chest, gasps dramatically, and collapses. The problem is that a pulmonary embolism rarely respects this theatrical script. Many patients sit at home waiting for agonizing, crushing pain before they take their symptoms seriously. They assume a mild, nagging ache in the ribcage is just a pulled muscle from yesterday's workout. It is not. In reality, a blood clot in the lungs can present as a faint, elusive pleuritic discomfort that only worsens when you take a deep breath. Because the discomfort mimics simple costochondritis or a minor respiratory bug, people swallow ibuprofen and go to sleep. That decision can be fatal.
Ignoring the root of the problem
Are there warning signs before a pulmonary embolism? Absolutely, but they frequently manifest below the pelvic floor. People blissfully ignore a swollen, throbbing calf because they think they merely strained it during a weekend jog. Up to 70 percent of pulmonary embolisms originate from deep vein thrombosis in the lower extremities. Yet, we treat the leg and the lung as entirely separate entities. You might notice one ankle looks slightly puffier than the other, or experience a deep ache that feels like a stubborn cramp. If you apply a vigorous massage to that area to "work out the knot," you might actually dislodge the thrombus. As a result: the clot travels straight to your pulmonary arteries.
The fitness fallacy
Healthy people do not get clots, right? Wrong. Marathon runners and elite cyclists frequently fall victim to this cardiovascular trap. Their resting heart rates are low, their muscles are highly conditioned, and they assume their bodies are invincible. Except that intense endurance training combined with long-distance travel to competitions creates the perfect storm for stagnation. When an athlete experiences sudden shortness of breath during a routine training session, they often attribute it to overtraining or seasonal allergies. They push through the invisible barrier. This stubborn resilience obscures the brewing crisis until the respiratory system completely fails.
The hidden trigger: Estrogen and the coagulation cascade
The hidden risk of hormonal fluctuations
Let's be clear about a major blind spot in modern triage: reproductive health. Medical literature often mentions oral contraceptives as a baseline risk factor, but the nuance is frequently lost in brief clinical consultations. Combined hormonal pills containing third- and fourth-generation progestins elevate the danger significantly. These specific formulations can increase the baseline risk of thromboembolism by almost fourfold compared to non-users. When a young woman arrives at an urgent care clinic complaining of a rapid heartbeat and slight dizziness, physicians who overlook her pharmacological history might dismiss the episode as a simple panic attack. (We see this diagnostic bias play out in emergency rooms far too often.) The issue remains that estrogen alters the delicate balance of clotting factors in the liver, turning a routine physiological process into a hypercoagulable nightmare.
The silent threat of dehydration and flight times
Consider the mundane reality of a international business flight. You sit in a cramped economy seat for nine hours, sipping complimentary gin and tonics while the cabin air strips your body of moisture. Air travel exceeding four hours doubles the likelihood of developing a venous thromboembolism during the subsequent weeks. The blood thickens, the calf muscles remain completely immobile, and the venous pumps stall. If you ignore the subtle heaviness in your thighs upon landing, you are missing the primary window for intervention. Why do we treat movement during travel as an optional luxury rather than a physiological necessity?
Frequently Asked Questions
Can a pulmonary embolism happen suddenly without any warning signs?
Yes, sudden death can be the very first manifestation of a massive saddle embolism in approximately 25 percent of all cases. However, retroactively analyzing patient histories usually reveals that subtle anomalies were present days before the catastrophic event. A minor bout of unexplained breathlessness during a short walk or a brief spell of lightheadedness is often rationalized away by the patient. Clinical data indicates that nearly 30 percent of individuals who survive a major embolic event recall experiencing localized calf pain or unusual fatigue in the preceding week. The signs were there, but they were simply too quiet to trigger alarm bells.
How long can you have a pulmonary embolism before it becomes fatal?
The timeline is completely unpredictable and depends entirely on the size of the clot and the baseline health of your right ventricle. A massive occlusion blocking the main pulmonary trunk can induce right-sided heart failure and death within minutes of the initial occlusion. Conversely, a series of subsegmental micro-clots can shower the lungs over several weeks, causing progressive damage that mimics chronic asthma. Medical registries show that the mortality rate drops below 10 percent if standard anticoagulant therapy is initiated promptly within the first few hours of symptom onset. Delaying diagnosis by even twenty-four hours exponentially increases the risk of sudden cardiac arrest.
Does an elevated heart rate always indicate a blood clot in the lungs?
Sinus tachycardia is a classic finding, but it is far from an exclusive indicator of a vascular blockage. Your heart accelerates due to anxiety, dehydration, fever, or a double shot of morning espresso. Statistically, a heart rate exceeding 100 beats per minute is observed in roughly 70 percent of confirmed embolic cases, making it a highly sensitive but poorly specific diagnostic marker. The true warning sign is a heart rate that remains stubbornly elevated while you are completely at rest in a cool room. When unexplained tachycardia accompanies a drop in oxygen saturation below 95 percent on a standard pulse oximeter, the clinical suspicion must immediately shift toward an acute vascular obstruction.
A definitive stance on vascular vigilance
We must abandon the passive expectation that a cardiovascular crisis will always announce itself with a dramatic flare. The human body communicates in whispers far more often than it screams, which explains why so many preventable deaths occur every single year. Waiting for a textbook combination of hemoptysis, chest pain, and severe dyspnea is a dangerous gamble that nobody should be playing. You need to become an uncompromising advocate for your own vascular integrity, especially if you possess known predisposing factors. Demanding a D-dimer blood test or a lower extremity ultrasound when you feel that something is fundamentally amiss is not hypochondria; it is rational self-defense. If the medical establishment occasionally minimizes your vague symptoms, you must hold your ground because the alternative is a silent catastrophe that leaves no room for second chances.