The Fluctuating Baseline: Unmasking What Aggravates Parkinson's Beyond Simple Genetics
Parkinson's disease does not march forward in a perfectly straight, predictable line. The thing is, patients and caregivers often mistake a temporary flare-up caused by a secondary issue for a permanent advancement of the underlying neurodegenerative process. James Parkinson himself, back in his 1817 monograph in London, noted how external influences seemed to whip up the tremors of his patients, yet modern clinics sometimes forget this clinical nuance. We see a sudden uptick in bradykinesia and immediately assume the brain has lost more substantia nigra neurons. We're far from it in many cases.
The Myth of Linear Progression
The brain's ability to cope with dopamine depletion is incredibly fragile. When a secondary stressor enters the mix, the central nervous system essentially undergoes a short circuit. Why does a minor cold make a patient's legs freeze to the kitchen floor? It happens because systemic inflammation temporarily breaches the blood-brain barrier, altering the pharmacokinetics of existing therapies. Experts disagree on the exact molecular threshold where this vulnerability peaks, but the clinical reality is undeniable.
Where It Gets Tricky with Symptoms
Distinguishing between actual neurodegenerative decay and a transient spike in symptom severity requires meticulous observation. A patient in Miami might experience a severe worsening of rigidity during a humid July heatwave, not because their disease suddenly mutated, but because acute dehydration drastically reduces the absorption efficiency of oral levodopa in the small intestine. It is a mechanical failure, not a structural one.
Chemical Sabotage: How Common Medications and Infections Trigger Rapid Decline
The chemical equilibrium in a brain dealing with Parkinson's is remarkably easy to disrupt. If you introduce the wrong molecule—even one meant to treat a completely unrelated ailment like nausea or heartburn—the results can be catastrophic. This is where medical oversight sometimes fails, as non-neurology specialists prescribe common drugs without realizing they are dumping fuel on a neurological fire.
The Anti-Dopaminergic Minefield in Modern Pharmacies
Certain standard medications act as silent antagonists to Parkinson's therapies. Take metoclopramide, a incredibly common drug prescribed for gastrointestinal motility issues, or traditional antipsychotics like haloperidol. These compounds blindly bind to D2 dopamine receptors. They lock them down. As a result: the carefully calibrated dose of carbidopa-levodopa a patient took an hour ago is rendered completely useless because the receptors are already occupied by an intruder. It takes just one dose of an incorrect antiemetic in an emergency room setting to induce a state of severe, terrifying rigidity that looks exactly like a massive disease acceleration.
Silent Infections and the Inflammatory Cascade
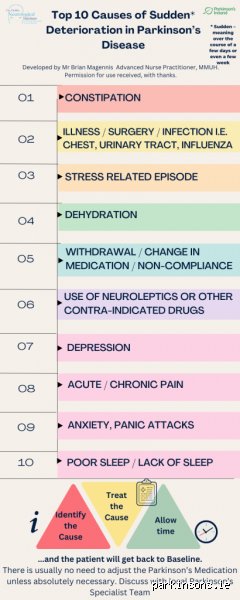
Infections are perhaps the most notorious culprits behind sudden clinical worsening. A 2022 study tracking 1,500 patients in neurological wards demonstrated that urinary tract infections (UTIs) and bacterial pneumonia accounted for over 40 percent of acute, non-stroke-related hospitalizations for Parkinson's exacerbations. The mechanism is a massive systemic cytokine release. These inflammatory proteins travel through the bloodstream and amplify neuroinflammation in the basal ganglia, making existing tremors violently worse. The issue remains that these infections are often asymptomatic in older adults, lacking the classic burning sensation or fever, manifesting instead solely as sudden confusion and a total loss of mobility.
The Gut-Brain Axis: Dietary Traps and Digestive Stagnation
People don't think about this enough, but the stomach is essentially the gatekeeper of Parkinson's stability. Because oral levodopa must be absorbed in the proximal small bowel, anything that delays or blocks this transit directly aggravates the disease symptoms by starving the brain of its required dopamine precursor.
The Great Protein Competition
Dietary protein is a double-edged sword. Levodopa utilizes the large neutral amino acid (LNAA) transport system to cross both the intestinal wall and the blood-brain barrier. If a patient consumes a heavy ribeye steak or a high-protein shake concurrently with their medication, those dietary amino acids aggressively compete with the levodopa for those limited transport slots. The dietary proteins usually win. Except that this doesn't just delay the drug; it can cause a total "off" state where the patient becomes completely immobilized for hours, wondering why their medication suddenly stopped working.
Gastroparesis and Mechanical Delivery Failures
And then there is the structural issue of gut motility itself. Parkinson's intrinsically damages the enteric nervous system, leading to a condition called gastroparesis—a fancy term for a paralyzed stomach. When a capsule of levodopa sits in a stagnant stomach for three hours instead of moving quickly into the intestine, it degrades. The patient gets zero benefit. This creates a vicious cycle: poor motility aggravates the symptoms, and the worsening symptoms further slow down the gut.
Psychological Stressors and Cortisol Shocks
It is easy to compartmentalize Parkinson's as a purely physical, structural disease of the motor cortex, but emotional turmoil acts as a direct chemical accelerator of physical symptoms. The boundary between the mind's anxiety and the body's motor control is practically non-existent in this context.
The Cortisol and Epinephrine Surge
When a person experiences acute anxiety or prolonged psychological stress, the adrenal glands flood the system with cortisol and epinephrine. In a healthy individual, this triggers a standard fight-or-flight response. But in a brain where dopamine producing cells are already operating at a 70 percent deficit, this adrenaline surge completely overwhelms the remaining motor circuitry. Tremors that were barely noticeable during a quiet morning at home can become violent and uncontrollable during a stressful family argument or a frustrating driving experience in heavy traffic. Which explains why a patient might appear perfectly fine in a calm, controlled clinical environment but look remarkably debilitated when trying to navigate a chaotic airport terminal.
Sleep Deprivation as a Cumulative Aggravator
Poor sleep architecture is not just a symptom of Parkinson's; it is a major aggregator of it. During deep slow-wave sleep, the glymphatic system clears metabolic waste from the brain parenchyma. When REM sleep behavior disorder or frequent nocturnal awakenings truncate this process, the brain accumulates oxidative stress. A single night of less than four hours of sleep can reduce the clinical efficacy of a patient's next-day medication regimen by an estimated 30 percent, making every physical task feel monumental. Honesty, it's unclear whether the lack of sleep destroys the dopamine receptors' sensitivity or simply exhausts the compensatory motor pathways, but the next-day physical toll is undeniable.
Common misconceptions that quietly worsen the disease
The obsession with protein timing and dosing
Many patients believe they must completely banish protein from their dinner plates. Amino acids compete with levodopa for absorption across the blood-brain barrier, which is a physiological reality. Except that starving your muscles to fix your dopamine uptake is a losing battle. Muscle wasting—sarcopenia—strikes hard in later stages. Think about it: a frail body falls faster. The issue remains that patients starve themselves of lean meats based on internet forums, unintentionally accelerating their own physical decline. You need a strategic two-hour window around your medication doses, not absolute starvation.
The myth of the mandatory high-intensity burnout
Exercise acts as a neuroprotective shield. We hear this constant refrain from every neurologist. But let's be clear: dragging an exhausted body through a brutal, high-impact CrossFit session when your cortisol levels are already soaring does more harm than good. Extreme physical exhaustion induces massive oxidative stress. That stress fries the remaining dopaminergic neurons you are desperately trying to protect. What aggravates Parkinson's faster than sedentary behavior? Ironically, it is physical burnout driven by toxic guilt. But who actually tells patients to just take a walk instead?
Chasing the tremor while ignoring the gut
A shaking hand commands attention. Constipation, however, gets shrugged off as a minor inconvenience. This is a massive clinical blunder. Chronic constipation allows toxic metabolites to linger in the digestive tract, altering the gut microbiome and triggering systemic inflammation. When inflammation spikes, blood-brain barrier permeability increases, which explains why a backed-up digestive system directly exacerbates motor fluctuations and cognitive slowing.
The hidden culprit: Subtle micro-stressors
The neurotoxic price of chronic low-grade friction
We know sudden trauma shatters neurological stability. Yet, the insidious damage caused by daily, low-grade environmental and emotional friction goes unnoticed. Consider the constant exposure to traffic noise or the persistent anxiety of a strained relationship. These micro-stressors keep the sympathetic nervous system trapped in a perpetual fight-or-flight state. Cortisol levels remain elevated, disrupting sleep architecture and preventing the brain from clearing metabolic waste through the glymphatic system. It is during deep sleep that the brain flushes out alpha-synuclein aggregates. Deprive yourself of that deep rest through ambient stress, and you accelerate the degenerative cascade. Neurologists rarely ask about your noisy neighbors, (though perhaps they should start), despite the clear link between environmental chaos and symptom progression.
Frequently Asked Questions
Does a lack of specific vitamins accelerate the progression of Parkinson's?
Yes, deficiencies in specific micronutrients can significantly compromise neurological resilience. Clinical data reveals that roughly 70 percent of Parkinson's patients exhibit profound Vitamin D deficiencies, a state correlated with higher fall risks and accelerated cognitive decline. Furthermore, low levels of Vitamin B12 elevate homocysteine, a neurotoxic compound that damages vascular structures within the basal ganglia. When these cofactors drop, the brain lacks the necessary tools to mitigate normal oxidative stress. Maintaining these specific nutrient levels will not cure the underlying pathology, but neglecting them leaves your nervous system completely defenseless.
Can sudden medication changes cause permanent damage?
Abruptly altering your chemical regimen is incredibly dangerous. Suddenly halting or drastically slashing dopaminergic therapies can trigger a life-threatening crisis known as Parkinsonism-hyperpyrexia syndrome, which presents with a fever exceeding 40°C and severe muscle rigidity. This acute state causes severe rhabdomyolysis and acute kidney injury. Even smaller, unmanaged fluctuations in your daily dosing schedule cause rapid shifts in brain chemistry. These chaotic shifts accelerate the onset of permanent levodopa-induced dyskinesias. Consistency in receptor stimulation is what keeps the brain stable.
How much does chronic dehydration affect daily motor symptoms?
Dehydration acts as an immediate amplifier of both motor and non-motor symptoms. When total body water drops by as little as 2 percent, orthostatic hypotension worsens dramatically, causing a sudden systolic blood pressure drop of more than 20 mmHg upon standing. This leaves the brain starved of oxygen, causing instant dizziness, confusion, and a freezing of gait. Furthermore, a dry gastrointestinal tract completely stalls medication absorption. Your levodopa simply sits in the stomach, failing to reach the small intestine where absorption occurs, rendering your standard dose completely useless