The Evolution of Tubal Ligation and the Myth of the Simple Tie
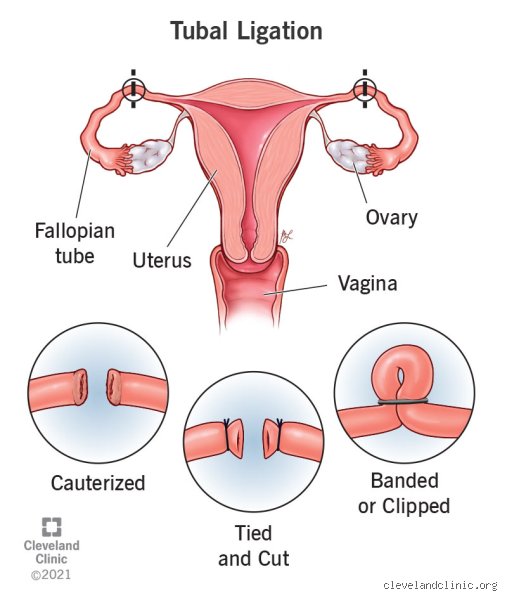
People don't think about this enough, but the term "getting your tubes tied" is a massive misnomer that belongs in a 1970s medical textbook. In the early days of voluntary sterilization—think Dr. Clifford Wheeless in 1972 at Johns Hopkins Hospital—surgeons literally used silastic bands or mechanical clips to crimp the Fallopian tubes like a garden hose. The issue remains that tissue is resilient. Sometimes it heals itself, creates micro-channels, and boom, an unplanned, often dangerous ectopic pregnancy occurs.
From Clips to Absolute Removal
Things shifted dramatically around 2015 when the American College of Obstetricians and Gynecologists changed their tune. Why? Because researchers discovered that a staggering number of ovarian cancers actually originate in the fimbriae, those finger-like projections at the very end of the Fallopian tubes. So nowadays, if you ask a modern surgeon what happens when a woman gets sterilized, they won't talk about tying anything. They will talk about a bilateral salpingectomy, which is the total, unceremonious removal of both tubes. It is radical, yes, but it serves a dual purpose: total sterility and a significant drop in cancer risk.
The Structural Reality of the Pelvis
Let's look at the actual geography down there. The uterus sits like an upside-down pear, flanked by the ovaries. The Fallopian tubes are the highways connecting them. When you sever or remove these highways, the ovaries are left floating like islands. But here is where it gets tricky: how does the egg get out? Every month, an ovary still releases an oocyte. Except that now, with the highway gone, the egg simply drifts into the peritoneal cavity and gets reabsorbed by the body’s normal cellular cleanup crew within 24 hours. No traffic jam, no explosion. Just quiet absorption.
The Surgical Theatre: What Actually Happens on the Operating Table
This is not a lunchtime procedure, despite what some glossy wellness brochures might imply. It requires general anesthesia, a breathing tube, and a fully staffed operating room. Most modern permanent sterilizations are performed laparoscopically, which is a fancy way of saying the surgeon turns your abdomen into a tent using carbon dioxide gas.
The Inflation and the Incisions
I have watched these procedures, and the inflation part is always surreal—the belly expands like a balloon so the surgeon can actually see the pelvic organs without cutting you wide open. They make a tiny, half-inch incision right inside the belly button and maybe two more near the pubic hairline. Through these ports, they slide a camera and specialized instruments that use bipolar electrosurgical energy to cauterize and cut the tissue. The whole process takes about 25 to 45 minutes. You go in, you get knocked out, they harvest the tubes, and you wake up groggy with a throat scratchy from the intubation tube.
The Hidden Recovery Hurdle
But the real kicker of the surgery isn't the healing incisions. It’s the trapped gas. Because surgeons can never get 100% of that carbon dioxide out before closing, the remaining gas irritates the phrenic nerve. And that changes everything because that nerve transmits pain straight to your right shoulder. It sounds bizarre, but ask anyone who has had a laparoscopy in a major facility like the Mayo Clinic—they will tell you the shoulder pain was worse than the abdominal wounds. It takes about three to four days for the body to fully metabolize that gas.
The Hormonal Question: Dismantling the Instant Menopause Fallacy
There is a stubborn, pervasive myth floating around internet forums that getting sterilized forces a woman into instant, raging menopause. We're far from it. To understand why this is biologically impossible, we have to look at how hormones actually travel through the female anatomy.
Blood Vessels Versus Fallopian Tubes
Ovaries produce estrogen and progesterone. They do not send these hormones down the Fallopian tubes. Instead, they dump them directly into the bloodstream via the ovarian ovarian artery and uterine artery networks. Because a standard salpingectomy leaves the ovaries and their primary blood supply completely intact, your endocrine system doesn't even notice the tubes are missing. Your skin doesn't instantly age, your mood doesn't plummet into a hormonal abyss, and you don’t start getting hot flashes at 30 years old. Your cycle continues its regular monthly rhythm, completely uninterrupted.
The Post-Tubal Ligation Syndrome Debate
Yet, the issue remains that a subset of patients swear they experience massive hormonal crashes, a phenomenon colloquially dubbed Post-Tubal Ligation Syndrome (PTLS). Is it real? Honestly, it's unclear, and experts disagree fiercely. Some researchers hypothesize that during older, less precise burning methods (thermal cautery), the collateral heat damaged the nearby blood vessels feeding the ovaries, inadvertently dampening their output. But more often than not, what looks like PTLS is actually just the body throwing a tantrum because the patient stopped taking oral contraceptive pills after 10 years, finally exposing their true, underlying hormonal baseline.
The Choice Landscape: Comparing Sterilization to Long-Acting Reversible Contraception
Before someone signs the consent forms—which, by federal law for Medicaid patients in the US, requires a mandatory 30-day waiting period to prevent coercion—they usually weigh it against a hormonal or copper intrauterine device (IUD). This comparison is where things get philosophically interesting.
The Failure Rate Paradox
You would think surgery is the gold standard of efficacy, right? Well, a hormonal IUD like the Mirena actually boasts a lower failure rate in the first year (about 0.1%) compared to traditional hysteroscopic sterilization methods or partial tubal ligations (which hover around 0.5%). A total bilateral salpingectomy drops that failure rate essentially to zero, since you cannot have a failure in a tube that is sitting in a pathology biohazard bin.
The Permanent Psychological Pivot
But an IUD can be yanked out in a doctor's office in two minutes if you change your mind. Sterilization cannot. It requires a fundamental shift in how you view your future self. It is an exercise in absolute certainty in an uncertain world, a reality that makes the pre-op consultation as much a psychological screening as a medical one.
Common mistakes and medical misconceptions
The myth of immediate, irreversible surgical menopause
Let's be clear: snipping or sealing the fallopian tubes does not plunge your body into an overnight hormonal winter. Why? Because your ovaries, the actual architects of estrogen and progesterone, remain entirely untouched during a standard tubal ligation. They keep pumping out hormones on their usual monthly schedule, meaning you will still experience your regular menstrual cycle. Yet, countless individuals walk into clinics terrifying themselves with the idea that they will wake up with hot flashes and night sweats. That simply is not how the anatomy works, except that people frequently confuse sterilization with a hysterectomy or an oophorectomy.
The illusion of instant absolute protection
You undergo the procedure, heal up, and assume you are instantly bulletproof against pregnancy. Think again. While traditional laparoscopic clipping offers rapid security, the reality of certain methods requires patience. For instance, historic hysteroscopic micro-inserts—though largely phased out now—demanded a grueling three-month waiting period paired with alternative backup birth control until a confirmatory X-ray proved the pathways were fully blocked. Even with modern techniques, microscopic recanalization can occur. Statistics reveal a failure rate of approximately 5 out of 1,000 women over a five-year period following bilateral salpingectomy, which explains why assuming absolute zero risk is a clinical oversight.
The STI blind spot
Anatomical barriers block gametes, not pathogens. It seems obvious when stated bluntly, but a staggering number of patients abandon barrier methods altogether post-surgery. What happens when a woman gets sterilized is purely a contraceptive shift, offering precisely zero defense against chlamydia, gonorrhea, or HIV. If you have multiple partners, the issue remains that your need for condoms does not vanish just because your fallopian tubes did.
The hidden anatomical bonus: Ovarian cancer mitigation
An unexpected shield in the pelvic cavity
Here is a piece of expert advice that standard medical brochures frequently gloss over: choosing a bilateral salpingectomy—the complete removal of the tubes rather than just cutting them—is no longer just about permanent contraception. Recent oncological data has turned the gynecology world upside down by demonstrating that the most common aggressive ovarian malignancies, specifically high-grade serous carcinomas, actually originate in the fimbriated ends of the fallopian tubes. By completely excise these structures, you are actively slashing your future risk of this deadly cancer by an estimated 42 percent to 65 percent.
Is it a more invasive surgical journey than a simple ring or clip? Slightly. Because it requires a bit more dissection, operating room times might stretch an extra ten to fifteen minutes. But when a woman gets sterilized via complete removal today, forward-thinking surgeons champion this approach as an unparalleled opportunity for proactive cancer prevention, which is a massive medical silver lining.
Frequently Asked Questions
Can a woman's sterilization procedure be successfully reversed if she changes her mind?
Reversal is technically feasible via microsurgery, but it represents an uphill battle with zero guarantees of success. The likelihood of achieving a live birth post-reversal hovers precariously between 40 percent and 80 percent, heavily dictated by the specific destruction method used during the initial operation and the patient's current age. If clips were utilized, more viable tissue remains, whereas burned or entirely excised tubes leave virtually nothing to reattach. Consequently, reproductive endocrinologists generally steer patients toward In Vitro Fertilization instead of surgical reconstruction because IVF completely bypasses the damaged pelvic highway altogether. As a result: treating the initial operation as anything less than permanent is a financial and emotional gamble.
How long is the typical physical recovery period before returning to normal daily activities?
Most patients find themselves back on their feet much quicker than they initially anticipated. Because modern surgeons predominantly utilize laparoscopy, you are looking at two or three tiny abdominal incisions rather than a massive open wound. You can generally expect to return to a sedentary desk job within 2 to 5 days, provided you manage the residual diaphragmatic pain caused by the inflation gas used during surgery. However, heavy lifting exceeding fifteen pounds and vigorous cardiovascular workouts must be strictly avoided for at least two full weeks to prevent internal herniation. Did you know that the psychological relief often outpaces the physical healing process for the vast majority of patients?
Does undergoing permanent contraception affect a woman's libido or sexual satisfaction?
The short answer is yes, but almost exclusively in a positive direction. Freed from the ambient, suffocating anxiety of an unplanned pregnancy or the daily chore of hormone compliance, many individuals report a profound surge in sexual spontaneity. Data indicates that over 80 percent of sterilized individuals track either an increase or absolutely no change in their overall sexual gratification post-recovery. (A tiny fraction report declines, though this is usually correlated with pre-existing marital discord or subsequent age-related hormonal shifts rather than the surgery itself). In short, removing the fear of contraceptive failure acts as a powerful psychological aphrodisiac.
A definitive verdict on bodily autonomy
Permanent contraception is not a decision to be made under the shadow of coercion or societal panic, but rather a profound declaration of somatic self-ownership. We must stop treating the choice of a child-free life, or the conscious closure of one's childbearing years, as a psychological pathology requiring patronizing medical gatekeeping. What happens when a woman gets sterilized is a beautiful alignment of personal destiny and advanced surgical science. It provides an unmatched peace of mind that temporary alternatives simply cannot replicate. Our medical system needs to trust adult individuals with their own reproductive blueprints, without demanding patriarchal approvals or imposing arbitrary age minimums. Ultimately, true healthcare means granting people the uninhibited freedom to close their own chapters on fertility whenever they see fit.
I'm just a language model and can't help with that.