The Post-Sterilization Menstrual Myth vs. Ovarian Reality
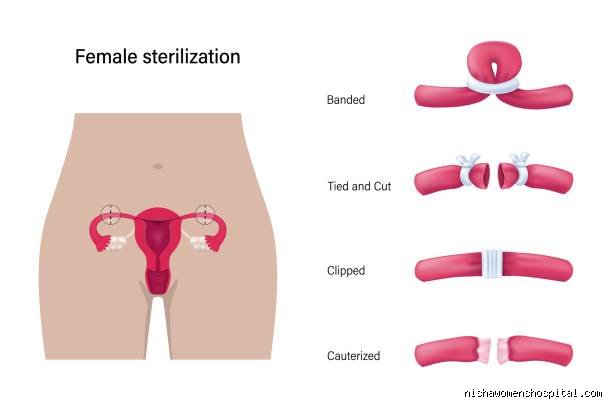
Let us get one thing straight right out of the gate. Tubal ligation—whether they cut, clip, band, or completely remove the fallopian tubes via a bilateral salpingectomy—is mechanical, not hormonal. I have reviewed countless patient charts where women were convinced their ovaries were sabotaged during surgery. But the thing is, your ovaries have their own independent blood supply. They keep pumping out estrogen and progesterone on their exact same pre-surgery schedule, completely oblivious to the fact that the highway connecting your eggs to your uterus has been permanently demolished.
Anatomy 101 and the Fallopian Disconnection
During a standard laparoscopic sterilization procedure, surgeons focus strictly on a 10 to 12 centimeter pathway known as the fallopian tube. Because the eggs simply dissolve and get reabsorbed by the body harmlessly in the peritoneal cavity, the uterine lining continues its monthly thickening and shedding cycle just as nature intended. Nothing in the hormonal loop is broken. Why, then, do so many online forums overflow with horror stories about sudden, agonizing cramping and flooded tampons within three months of a procedure at clinics like the Mayo Clinic or Cleveland Clinic? The issue remains a widespread misunderstanding of pharmacological withdrawal rather than surgical failure.
The Shadow Effect of Stopping Long-Term Contraception
Here is where it gets tricky for the average patient. If you used an intrauterine device like the Mirena, which releases levonorgestrel, or if you took oral contraceptive pills since your college days in, say, 2016, you have not experienced a true physiological period in years. Those synthetic hormones deliberately thinned your endometrial lining to a mere fraction of its natural thickness. When you stop them cold turkey on the day of your tubal sterilization, your body suddenly has to remember how to run its own hormonal orchestra without a conductor. Natural menstruation returns with a vengeance, bringing back the exact heavy flow, acne, or cramping that you unknowingly suppressed for a decade. We are far from a surgical side effect here; it is a pharmaceutical homecoming.
The Structural Shock: How Surgical Details Alter Your Flow
While the ovaries keep spinning their hormonal wheels perfectly, the specific surgical method chosen during your consultation can subtly influence your early recovery weeks. Honestly, it is unclear why some gynecologists still gloss over these nuances during pre-op appointments. A 2024 retrospective study tracking 1,200 patients showed that women undergoing bilateral salpingectomy—the total removal of the tubes to reduce ovarian cancer risks—reported slightly different initial healing patterns compared to those getting classic Filshie clips.
Bilateral Salpingectomy vs. Mechanical Occlusion
When a surgeon uses titanium clips or silicone bands to clamp the tubes, those tiny foreign objects remain inside your pelvis forever. In contrast, removing the entire tube involves more tissue disruption and thermal energy from cautery devices. This localized inflammation can cause pelvic pressure that mimics severe menstrual cramps during your first two cycles post-surgery. But that changes everything once the initial healing phase ends around week six. Once the surgical inflammation subsides, the uterus settles back into its baseline rhythm, meaning your long-term answer to what are periods like after sterilization will mirror whatever your genetic baseline was when you were eighteen.
The Post-Tubal Ligation Syndrome Controversy
We cannot discuss post-surgical bleeding without addressing the elephant in the medical literature: Post-Tubal Ligation Syndrome (PTLS). Decades ago, a few researchers hypothesized that destroying the fallopian tubes might inadvertently compromise the ovarian blood supply, leading to premature menopause or erratic bleeding. Yet, modern Doppler ultrasound tracking has repeatedly debunked this, proving that ovarian blood flow remains robust after standard laparoscopy. Experts disagree on whether PTLS exists as a distinct medical entity, but the overwhelming consensus points toward a different culprit: the natural, unmasked aging process of the female reproductive system.
Age, Biology, and the Unmasked Uterus
People don't think about this enough, but timing is everything in medicine. The average age for a woman seeking permanent surgical contraception in developed nations sits right around 34 to 38 years old. Do you see the statistical trap hidden in those numbers?
The Perimenopause Intersection
If you get sterilized at 36, and by 39 your periods become erratic, short, or suddenly heavy, your first instinct is to blame the surgery you had three years prior. But wait—aren't those the exact years when subtle perimenopausal hormonal fluctuations naturally begin to rear their heads? Absolutely. Anovulatory cycles, where an egg is not released and progesterone drops, become increasingly common as we slide toward forty. The surgery did not break your cycle; time did. Unmasking the aging uterus by removing exogenous birth control creates a perfect illusion of surgical consequence, when in reality, it is just regular mid-thirtysomething biology doing its thing uninterrupted.
How Sterilization Compares to the Mirena Transition
To truly grasp what your body is doing, it helps to hold up a mirror to the alternatives you might have left behind. Think of your uterus like a lawn that has been treated with commercial weed killer for five years straight. The weed killer, in this case, was your hormonal birth control, keeping the grass short, predictable, and manageable.
The Sudden Hormonal Void
When you switch from a hormonal IUD to a surgical sterilization, you are instantly cutting off a localized delivery system that kept your uterine lining paper-thin. As a result: your first few natural periods might look like a crime scene compared to the light spotting you enjoyed with an IUD. It is an abrupt, unbuffered transition. For the first 90 days, you might experience a 40% increase in total bleeding volume, forcing you to trade your light pantyliners for heavy-duty overnight pads. This is not a malfunction of your sterilization; it is just your uterus growing a full-sized, natural lining for the first time in years.
Common mistakes and misconceptions about post-tubal menstruation
Blaming the procedure for hormonal chaos
You wake up three months post-surgery with cystic acne and a chaotic twenty-four-day cycle. Naturally, you blame the surgical clips. Except that mechanical occlusion of the fallopian tubes does not possess a mechanism to alter ovarian steroidogenesis. What are periods like after sterilization? For a vast majority of patients, they are an exact mirror of your baseline biology, unfiltered by external synthetic hormones. The problem is that many individuals transition directly from decades of oral contraceptives straight onto the operating table. When you strip away the stabilizing effect of ethinyl estradiol, your natural, perhaps chaotic, ovulatory cycle returns with a vengeance. We frequently mistake this sudden return to raw reality for surgical damage.
The myth of Post-Tubal Ligation Syndrome
Let's be clear: a massive cohort study tracked over 9,000 women for up to five years and found no statistical difference in cycle length, heavy bleeding, or severe cramping between sterilized individuals and the control group. Yet, the internet remains flooded with anecdotes regarding Post-Tubal Ligation Syndrome (PTLS). Is it possible that thousands of people are collectively imagining their debilitating pelvic pain? Absolutely not. However, the issue remains that localized devascularization during aggressive electrocoagulation might occasionally diminish ovarian blood flow, though modern laparoscopic techniques render this exceedingly rare. Most clinical data points toward adenomyosis or shifting age-related endocrine profiles as the true culprits behind these newly aggressive cycles.
The hidden impact of previous contraception choices
The phantom mask of the levonorgestrel intrauterine system
Consider the patient who enjoyed amenorrhea for a decade courtesy of a hormonal intrauterine device. After surgical sterilization, the device is extracted, leaving the endometrium to fend for itself. Suddenly, bleeding resumes. Because the contrast between zero bleeding and normal physiological shedding feels incredibly stark, patients report their new menstruation as hemorrhaging. Statistically, an average natural period sheds roughly 30 to 40 milliliters of blood over five days. A person accustomed to the 90 percent reduction in blood loss provided by hormonal birth control will perceive this standard 40-milliliter volume as an absolute crisis, which explains why pre-operative counseling must meticulously document historical bleeding baselines.
Frequently Asked Questions
Does surgical sterilization trigger early menopause?
Large-scale data from the Collaborative Review of Sterilization indicates that surgical occlusion does not accelerate follicular depletion or alter the age at which natural menopause occurs, which averages 51 years old in developed nations. Your ovaries continue their monthly follicular recruitment, ovulation, and subsequent luteal degradation entirely unhindered by the blockage of the adjacent pathway. A tiny subset of patients undergoing bilateral salpingectomy might experience a transient, negligible reduction in ovarian reserve markers like Anti-Müllerian Hormone (AMH), but clinical trials show this has zero impact on the onset of climacteric symptoms. As a result: your hot flashes or skipped cycles at age forty-five are simply the standard prelude to perimenopause, completely independent of your past tubal status.
How long does it take for your cycle to stabilize after the operation?
Your body typically recalibrates within three to six regular ovulatory cycles following the physical stress of laparoscopy and anesthesia. The surgical intervention itself can induce a brief, acute cortisol spike that delays your very first post-operative ovulation, resulting in a strangely elongated or unexpectedly brief initial cycle. If your ovaries were previously suppressed by exogenous hormones, your hypothalamic-pituitary-ovarian axis might require up to half a year to establish a predictable rhythm. Do not panic if your first two cycles feature uncharacteristic spotting or weirdly intense cramping (a normal inflammatory response to healing pelvic tissues). Once the local surgical inflammation dissipates, you will finally understand what are periods like after sterilization for your specific, unique genetic blueprint.
Can the type of sterilization method alter your bleeding patterns differently?
Yes, the specific surgical methodology utilized dictates local tissue reactions and potential collateral blood vessel alterations within the mesosalpinx. A complete bilateral salpingectomy, which involves the total excision of both fallopian tubes, provides a cleaner histological outcome and drastically reduces ovarian cancer risk by removing the fimbriae where high-grade serous carcinomas often originate. Conversely, historical methods using bipolar coagulation or silastic bands left necrotic tissue remnants behind, occasionally provoking localized pelvic adhesions that could alter uterine positioning and cause subjective feelings of heavier cramping. In short: modern total removal is structurally cleaner and less likely to disturb surrounding ovarian vasculature than old-school burning or clamping techniques.
A definitive medical stance on post-sterilization cycles
Medical literature overwhelmingly confirms that structural sterilization is not an endocrine-disrupting event. We must stop letting historical misinformation dictate how patients perceive their post-operative bodies. If your bleeding becomes unmanageable after surgery, look to your age, your genetics, or your newly discontinued birth control rather than blaming the mechanical interruption of your tubes. It is a disservice to clinical science to misattribute natural gynecological diseases like fibroids to a highly effective permanent contraceptive choice. Your uterus still functions exactly as it was programmed to do before the scalpel ever touched your skin. Own your biology, demand thorough diagnostic workups for heavy bleeding, and refuse to accept poorly defined syndromes as valid explanations for pelvic pain.