The Anatomy of the Decision: What Female Sterilisation Actually Entails Beyond the Jargon
People don't think about this enough, but when we talk about getting your tubes tied, we are discussing a permanent alteration of your reproductive superhighway. The biological objective is simple: blocking the fallopian tubes so egg and sperm can never share a cosmic high-five. Yet, the path to achieving this is where it gets tricky because the medical community throws around terms like tubal ligation, salpingectomy, and occlusion as if they are interchangeable. They are not.
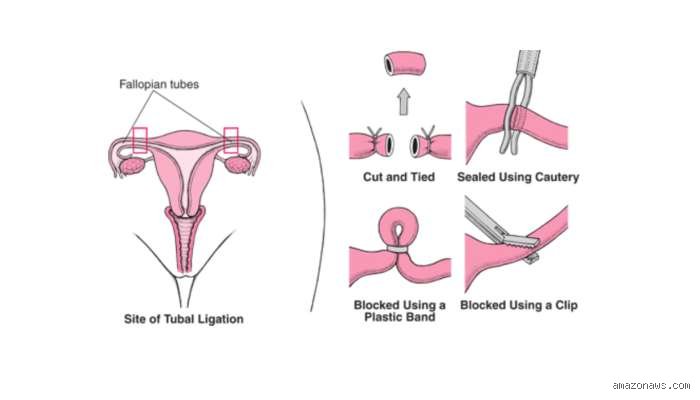
The Classic Tubal Ligation vs. The Modern Total Salpingectomy
For decades, the standard operation involved clamping, cutting, or burning the fallopian tubes—a method known as a traditional tubal ligation. The issue remains that leaving the remnants of the tubes behind carries a tiny, lingering failure rate and, interestingly, a higher risk of certain ovarian cancers that actually start in the tubal tissue. Which explains why back in 2015, the American College of Obstetricians and Gynecologists shifted its stance. Now, many surgeons in clinics from Chicago to London prefer a total salpingectomy—the complete and utter removal of the tubes. I think this shift is entirely justified given the oncology benefits, even if it means a slightly longer time on the operating table. Does removing the entire organ cause more post-operative agony than just clipping it? Surprisingly, clinical audits show the recovery pain profiles are almost identical, except that you are trading a few days of localized inflammation for lifetime peace of mind.
The Historical Ghost of Essure and Non-Surgical Occlusion
We cannot talk about the spectrum of pain without mentioning hysteroscopic sterilisation, specifically the now-defunct Essure device. Inserted through the cervix without incisions, these micro-inserts triggered chronic pelvic pain and inflammation in thousands of women before being pulled from the global market in 2018. It was a dark chapter that proved "non-invasive" does not always equate to painless. Today, surgical intervention remains the gold standard, forcing patients to confront the reality of the scalpel.
Decoding the Ouch Factor: Dissecting Laparoscopic Surgical Pain Step by Step
The vast majority of modern sterilisations are performed via laparoscopy—often called keyhole surgery—under general anaesthesia. You will sleep through the actual cutting, of course. But the moment the narcotics wear off in the recovery room, reality hits. And that reality has a very specific, bizarre flavor that catches many patients completely off guard.
The Ghost Pain: Why Your Shoulders Hurt After Belly Surgery
This is where conventional wisdom fails because the sharpest pain you might feel during the first 48 hours is not even in your abdomen. To see your reproductive organs clearly, the surgeon must inflate your peritoneal cavity with carbon dioxide gas. Though they aspirate most of it out before suturing you up, trapped gas pockets inevitably remain. This residual gas irritates the phrenic nerve, which shoots a sharp, stabbing sensation straight up to your right shoulder blade. It feels exactly like you have thrown out your back during a violent gym session, a phenomenon that confounds patients who expected only uterine cramps. Walking around the living room like a turtle is ironically the only way to dissipate this gas, as standard painkillers do very little to soothe a trapped bubble.
The In-The-Trenches Abdominal Cramping
Beneath the shoulder discomfort lies the localized pelvic trauma. Your uterus has been manipulated, your fallopian tubes have been severed or removed entirely, and your abdominal wall has been punctured in two or three places. Expect a deep, heavy throb that mimics the worst menstrual period of your life, compounded by sharp, stinging sensations whenever you twist your torso or laugh. At the Mayo Clinic, post-operative tracking indicates that while 85 percent of patients manage this with a combination of ibuprofen and acetaminophen, a small fraction require stronger opioids for the first two nights. The thing is, everyone heals at an unpredictable pace.
Incision Site Soreness and the Intubation Hangover
Then there are the minor insults to the body. The small incisions—usually one hidden inside the belly button and another near the pubic hairline—will itch, throb, and bruise. Furthermore, you will likely wake up with a raw, scratching throat caused by the endotracheal tube that breathed for you while you were under. It is a symphony of minor discomforts rather than one overwhelming agony, but when combined, that changes everything about your first weekend of recovery.
The Alternative Route: Laparotomy, Postpartum Sterilisation, and Hysterotomy Realities
Not everyone gets the luxury of tiny keyhole incisions. The physical toll of the procedure alters dramatically if the entry method changes, particularly if the sterilisation is piggybacked onto another major medical event.
The Post-Caesarean Section Tubal Ligation
A massive portion of sterilisations occur immediately after a woman gives birth via C-section. Since the obstetrician is already inside the abdomen, adding a tubal ligation takes mere minutes. But honestly, it is unclear where the birth recovery ends and the sterilisation pain begins in this scenario. Your uterus is already contracting violently to return to its normal size, and you are healing from a major 10-to-15-centimetre uterine incision. In this context, the added pain of the sterilisation itself is largely masked by the larger abdominal trauma, yet the overall healing timeline stretches out to a grueling six weeks.
The Mini-Laparotomy Post-Vaginal Delivery
If you choose to get your tubes tied within 24 to 48 hours after a successful vaginal delivery, the surgeon will likely perform a mini-laparotomy. They make a small incision just below the navel, which is still riding high because the uterus has not shrunk back down yet. But here is the kicker: your body has just endured the marathon of childbirth, and now you are heading back into surgery. The physical exhaustion exacerbates pain perception, making the recovery feel significantly more intense than it would on a random Tuesday when you were well-rested.
The Pain Ledger: How Sterilisation Compares to Long-Acting Reversible Contraception
When weighing how painful is female sterilisation, we must look at the alternatives, because avoiding the operating room does not mean avoiding discomfort. The comparison is stark, featuring completely different types of physical endurance.
The Sharp Shock of IUD Insertion
Many women opt for a hormonal or copper Intrauterine Device (IUD) to avoid permanent surgery. The pain of an IUD insertion is infamous—a sharp, blinding, localized agony that lasts for about 30 seconds as the cervix is clamped and the device is pushed into the uterine fundus, often followed by weeks of erratic cramping. Compared to sterilisation, the IUD offers a massive burst of acute pain that fades rapidly. Sterilisation, conversely, trades that single flash of agony for a prolonged, multi-day dull throb. But once those five days of surgical recovery are over, the pain ledger resets to zero forever, whereas IUD users often battle cyclic cramping for months.
Vasectomy: The Elephant in the Room
We cannot ignore the gender disparity here. A vasectomy is a non-invasive, outpatient procedure done under local anaesthetic in a urologist's office, taking roughly 20 minutes with a recovery time that involves a bag of frozen peas and two days on the couch. Female sterilisation requires entry into a sterile operating theatre, general anaesthesia, and the breaching of the peritoneal cavity. It is undeniably more painful, riskier, and requires a vastly more demanding physical sacrifice than male sterilisation, a biological tax that couples must weigh heavily before deciding who gets benched.