The Complex Mechanics Behind Why an Erection Loses Its Stamina
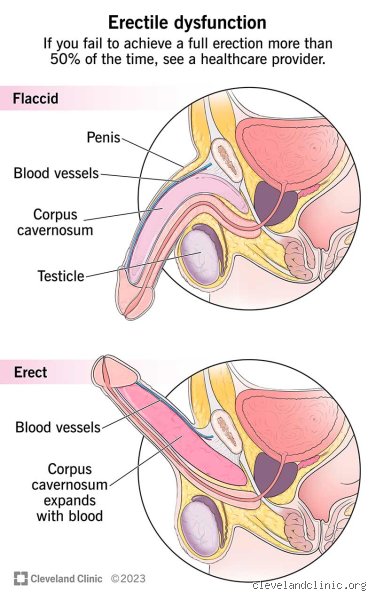
We tend to view the erection as a simple hydraulic lever, but the truth is far more annoying. It requires a massive influx of blood trapped under high pressure within two sponge-like chambers called the corpora cavernosa. If your heart cannot pump efficiently, or if the tiny blood vessels leading to the pelvic region are compromised, the pressure drops. And that changes everything.
The Vascular Highway and Nitric Oxide Production
The thing is, erectile health is fundamentally cardiovascular health, just on a much smaller, more fragile scale. When a man becomes aroused, the endothelial cells lining his pelvic arteries release a tiny gas molecule called nitric oxide. This molecule tells the smooth muscle tissue to relax, allowing blood to rush in at a rapid clip. But if you have early-stage atherosclerosis—a condition where plaque builds up in the arteries—the penile arteries, which are a mere 1 to 2 millimeters in diameter, clog long before the much larger coronary arteries do. This explains why a sudden, unexplained soft erection can actually be the very first warning sign of underlying heart disease, sometimes beating a heart attack to the punch by as much as three to five years. Think of it as the canary in the cardiovascular coal mine.
Neurological Misfires and the Brain-Body Disconnect
But what happens when the pipes are clean yet the signal still fails to arrive? That is where the nervous system comes in. The brain must send a clean, uninterrupted electrical impulse down the spinal cord through the pelvic splanchnic nerves to initiate the whole chemical cascade. If you have a condition like multiple sclerosis, or perhaps you sustained nerve damage during a past pelvic surgery—prostatectomies are notorious for this—the pathway is severed. The desire is fully present in the mind, yet the physical destination remains completely offline. It is an incredibly frustrating disconnect, honestly, and it highlights just how dependent the anatomy is on pristine neurological wiring.
The Physiological Culprits: From Metabolic Chaos to Hidden Vascular Leaks
People don't think about this enough, but metabolic diseases are absolute killers when it comes to sexual performance. Take type 2 diabetes, for instance, which effectively delivers a double whammy to the groin by simultaneously damaging both the delicate nerve endings and the microvasculature. Statistics from the Cleveland Clinic show that up to 75% of men with diabetes will experience some degree of erectile dysfunction over their lifetime, often developing it a decade earlier than their healthy peers. High blood sugar acts like microscopic shards of glass, slowly shredding the very infrastructure required to maintain rigidity.
The Venous Leak Nightmare
Where it gets tricky is a phenomenon known as a veno-occlusive dysfunction, or more colloquially, a venous leak. Even if your arteries are wide open and pumping blood into the penis like a firehose, you still cannot maintain an erection if the exit valves fail to close. In a healthy scenario, the expanding sponge tissue compresses the penile veins against a rigid outer sheath, trapping the blood inside. But if that tissue loses its elasticity due to aging, low testosterone, or physical trauma, the blood slips right back out into the general circulation as fast as it entered. Why does this happen? The issue remains a subject of intense debate among urologists, but structural degradation of the tunica albuginea is the primary suspect. You are essentially trying to inflate a tire that has a nail driven straight through the sidewall.
The Chemical Cocktail of Modern Pharmaceuticals
Sometimes, the enemy is sitting right inside your medicine cabinet. A massive array of commonly prescribed medications list erectile dysfunction as a primary side effect, yet doctors rarely emphasize this during a brief fifteen-minute consultation. Beta-blockers prescribed for hypertension, for example, intentionally slow the heart rate and lower blood pressure across the entire body. Which explains why your pelvic region suddenly lacks the sheer hydraulic force required for intimacy. Antidepressants, specifically Selective Serotonin Reuptake Inhibitors like sertraline or fluoxetine, alter brain chemistry to manage anxiety, but they also inadvertently blunt the dopaminergic pathways that trigger sexual arousal in the first place. You fix the mood, but you break the mechanics. It is a cruel trade-off.
The Psychological Quagmire: When the Brain Short-Circuits the Body
We cannot talk about what causes a penis to be weak without addressing the massive, anxious elephant in the room. The human brain is the ultimate sex organ, possessing the absolute power to veto any physical arousal loop via the chemical release of adrenaline and cortisol. When you are stressed about performance, finances, or relationship friction, your sympathetic nervous system—the ancient "fight or flight" mechanism—takes total control of your body. Adrenaline instantly constricts peripheral blood vessels to redirect blood toward your lungs and major muscle groups so you can hypothetically run away from a saber-toothed tiger. Except that there is no tiger; there is just a very stressed man in a bedroom, and you cannot get an erection when your body thinks it is fighting for survival. We are far from achieving a relaxed state in those moments.
Performance Anxiety and the Spectatoring Trap
Once a single failure occurs, a vicious psychological loop begins. A man starts "spectatoring," a term coined by sexologists to describe the act of mentally stepping outside of one's own body during sex to critically analyze the erection's progress. Are you actually enjoying the moment if you are constantly monitoring your own rigidity like a scientist checking a gauge? No. This hyper-awareness triggers another spike of cortisol, ensuring the erection softens further, thereby confirming the man's worst fears and cementing the anxiety for the next encounter. I have seen this destroy the confidence of otherwise perfectly healthy 25-year-old men whose vascular systems are entirely flawless. The problem is not in the pelvis; it is a software glitch overriding perfectly good hardware.
Vascular Failure vs. Psychogenic Weakness: The Telling Differences
Teasing apart whether a weak erection stems from a damaged body or an anxious mind is the first critical step in any clinical evaluation. The diagnostic divergence is usually quite stark, yet many men overlook the obvious clues. Psychogenic ED typically hits like a lightning bolt—sudden, unpredictable, and highly situational. One night everything works perfectly, and the next, perhaps with a new partner or after a stressful day at the office, the system completely crashes. Vascular ED, however, is a slow, agonizing crawl that takes months or years to manifest, gradually stealing away morning erections and reducing rigidity across all scenarios, whether a partner is present or not.
The status of your nocturnal penile tumescence—the involuntary erections that occur during REM sleep—tells the real story. The average healthy male experiences between three to five erections per night, a biological maintenance routine designed to oxygenate the pelvic tissues. If you wake up with standard rigidity but find yourself softening during intimacy, your vascular pathways are clearly intact, pointing the finger squarely at anxiety or relationship dynamics. But if the morning erections vanish entirely for months on end, the plumbing is compromised. The tissue is starving for oxygenated blood, hence the progressive decline in daytime performance. Experts disagree on the exact timeline for intervention, but ignoring a total absence of nocturnal erections for more than six months is an excellent way to turn a treatable vascular issue into permanent structural damage.