The Day-One Reality of Permanent Birth Control Procedures
You wake up in a recovery room, throat dry from the breathing tube, your abdomen feeling like you performed a thousand sit-ups without training. The thing is, we treat modern sterilization as a minor blip in a workweek, but your body registers it as a distinct trauma. Whether a surgeon clamped your fallopian tubes or snips were made to your vas deferens, tissue was severed. Dr. Aris Tsigris, a renowned pelvic surgeon practicing in Athens, noted during a 2024 reproductive health summit that nearly forty percent of patients underestimate the systemic exhaustion that follows general anesthesia.
The Immediate Post-Operative Hours
Gas pain is the hidden villain here. During a laparoscopic tubal occlusion—which remains the gold standard for female sterilization—the surgical team inflates the abdomen with carbon dioxide gas to create a clear workspace. But where it gets tricky is that this gas does not just vanish when they stitch you up. It traps itself beneath the diaphragm, irritating the phrenic nerve and radiating directly into your right shoulder. People don't think about this enough, expecting incision pain but instead getting a bizarre, sharp ache in their neck while trying to sip ginger ale. Walking around the living room helps expel it, yet the first twelve hours are mostly spent drifting between nap cycles and wondering why your shoulder hurts more than your pelvis.
Deconstructing the Surgical Trajectory: Tubal Ligation versus Vasectomy
We need to stop grouping these two operations into the same recovery bucket because doing so creates massive architectural misunderstandings about healing timelines. A vasectomy is an external, elegant, almost bloodless scalpel-free puncture performed under local numbing blocks. Conversely, a female sterilization requires entering the peritoneal cavity. That changes everything. To pretend a man ice-packing his scrotum for forty-eight hours faces the same biological toll as a woman whose fallopian tubes were burned with bipolar coagulation is medically absurd.
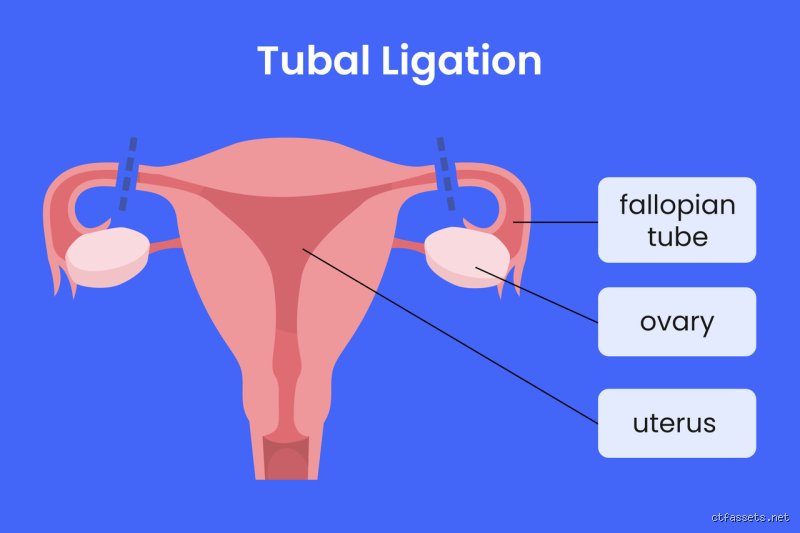
The Intricacies of Laparoscopic Healing
When looking closely at the recovery after sterilization for women, the entry points dictate the discomfort. Most surgeons utilize a two-port system: a ten-millimeter incision hidden neatly inside the belly button and a smaller five-millimeter puncture just above the pubic hairline. These tiny wounds are closed with absorbable sutures or medical glue, meaning you will not have the anxiety of someone pulling threads out of your skin a week later. Yet, internal healing operates on its own stubborn schedule. The uterine ligaments were manipulated during the procedure, which explains why many women experience vaginal bleeding similar to a moderate menstrual period for up to seventy-two hours post-surgery. Experts disagree on whether strict bed rest accelerates this phase, but honestly, it's unclear if horizontal stagnation does anything other than make your lower back ache.
The External Simplicity of Male Occlusion
For men, the trajectory is mercifully shorter but carries its own hyper-specific set of rules. The vas deferens are isolated, cut, and often cauterized through a single opening that rarely requires more than a single stitch. But do not let that simplicity trick you into running a marathon on day three. The scrotum lacks structural tissue support; hence, gravity becomes your primary enemy during the initial phase of recovery after sterilization. If you skip wearing a supportive jockstrap and choose loose boxers instead, the weight of the testes pulls on the healing vasa, inducing a deep, sickening ache that throbs through the inguinal canal. A clinical review published in the Journal of Urology highlighted that fifteen percent of vasectomy failures or complications stem not from surgical error, but from men lifting heavy objects within the first week.
Managing the Invisible Milestones of Early Convalescence
By day three, the initial fog of the surgical suite lifts, leaving you to navigate the mundane mechanics of daily life. Can you shower? Yes, usually after twenty-four hours, provided you do not scrub the surgical sites or submerge your torso in a bath. Except that people frequently forget how much core strength it takes simply to stand upright under streaming water while dealing with a lingering narcotics hangover. But what about the emotional shift? I have observed that the sudden realization of permanent infertility triggers an unexpected, brief psychological dip in a small fraction of patients—even those who were entirely certain of their choice.
The Paradox of Pain Management
The issue remains that we are currently caught in an aggressive cultural pivot away from opioid prescriptions, which means you will likely be sent home with instructions to alternate ibuprofen and acetaminophen. For the vast majority, this works beautifully. Yet, a blanket refusal to prescribe stronger analgesics for the first night can leave patients with lower pain tolerances stranded in agonizing discomfort. A study out of the Mayo Clinic tracked post-sterilization pain metrics and found that while eighty-five percent of patients managed successfully with over-the-counter anti-inflammatories, the remaining fifteen percent required a rescue dose of tramadol to break the pain cycle. It is a fine line between avoiding dependency risks and practicing basic medical empathy.
Navigating the Immediate Alternatives and Fail-Safes
We are far from the days when sterilization meant major open laparotomies and week-long hospital stays. However, looking at the recovery after sterilization demands that we contrast it against the transition periods of other long-acting reversible contraceptives. When someone removes a hormonal intrauterine device to undergo surgical permanent contraception, their endocrine system experiences a sudden, turbulent reset. They are not just healing from incisions; they are crashing from progesterone withdrawal. Did your doctor warn you about that potential mood rollercoaster mid-recovery? Probably not.
The Post-Vasectomy Clearance Window
Here is where a vital piece of conventional wisdom needs a sharp correction: you are not sterile the moment you walk out of the vasectomy clinic. This is a massive trap that leads to thousands of unplanned pregnancies globally. Viable spermatozoa remain trapped in the storage reservoirs of the seminal vesicles downstream from the surgical cut. As a result: you must utilize a secondary form of birth control for at least twelve weeks or until you have logged at least twenty ejaculations. A laboratory technician must view your semen sample under a microscope to confirm total azoospermia before you can discard your condoms. In short, the physical recovery after sterilization might take a weekend, but the functional confirmation of your sterility requires months of patient compliance.