The Hidden Reality Behind High-Level Surface Decontamination
People don't think about this enough: a single percentage point shift in your raw chemical bottle changes everything. We routinely throw around terms like sterilization and sanitization without realizing that a high level disinfection 1000 ppm protocol sits in a very particular, high-stakes medical and industrial niche. I have watched experienced lab managers eyeball their mixtures, oblivious to the fact that their baseline concentrate had degraded sitting on a sunny loading dock in Miami. The EPA clarifies that high-level disinfection traditionally implies the destruction of all vegetative microorganisms, mycobacteria, viruses, and fungal spores. Yet, it might not kill every last stubborn bacterial endospore—that is the job of actual sterilization autoclaves.
Why Parts Per Million Dictates Clinical Safety
What does 1000 ppm actually mean when we strip away the lab coats and jargon? It represents 1000 milligrams of active, free available chlorine per liter of water. When dealing with highly infectious environments—think of a Norovirus outbreak at a commercial cruise terminal or cleaning up a blood spill in an oncology clinic—skimping on this concentration leaves viable viral particles behind. Conversely, overshooting the mark corrodes expensive stainless steel medical equipment and off-gases toxic fumes that send your staff running for the exits. The math must be flawless because the biological margin for error is effectively zero.
Decoding the Math: Calculating Your Chlorine Mix Ratio Step-by-Step
Where it gets tricky is that the jug of bleach you buy at the distributor does not come labeled with instructions for a high level disinfection 1000 ppm solution. You are forced to calculate the dilution factor based on the initial concentration of sodium hypochlorite. Let us break down the standard formula using basic algebraic cross-multiplication, which works regardless of whether you handle metric liters or imperial gallons.
The Universal Dilution Formula for Chlorine Solutions
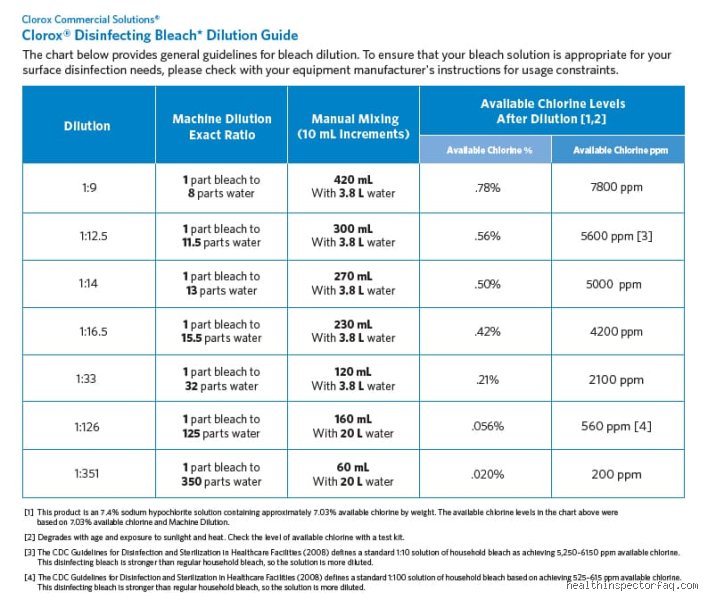
To find your dilution factor, you take the percentage of sodium hypochlorite in your bottle and multiply it by 10,000 to convert that percentage directly into parts per million. For instance, a standard 5.25% bottle equals 52,500 ppm of raw chlorine. Next, you divide this initial strength by your target strength, which in this specific case is 1000. When you divide 52,500 by 1000, you get a dilution factor of 52.5. This means your total final volume must be 52.5 times the volume of the bleach you started with. To simplify this for frontline environmental services staff, you round slightly to a clean 1:50 mix ratio—meaning 1 part chemical to 50 parts clean water.
Adjusting for Concentrated 6% and 8.25% Formulations
But what happens when your supply chain substitutes a high-strength 8.25% institutional concentrate? If you blindly stick to the old 1:50 rule, you will end up creating a harsh 1650 ppm solution that ruins surfaces and burns throats. For an 8.25% bottle, the math dictates dividing 82,500 by 1000, yielding a dilution factor of 82.5, which translates to roughly 1 part bleach to 82 parts water. It is a massive variance. Honest administrators admit that keeping track of these moving targets across multiple facility departments is a logistical nightmare because manufacturers frequently alter their concentrations without changing the front label design.
The Role of Water Quality and Temperature in Chemical Stability
You can calculate the perfect mix ratio for a high level disinfection 1000 ppm protocol on paper, but the water coming out of your facility faucet might completely derail your efforts. Hard water contains high levels of dissolved calcium and magnesium ions. These minerals naturally bind to the hypochlorite molecule, rendering a significant portion of the chlorine completely inert before it even touches a contaminated counter.
The Unseen Impact of pH and Dissolved Minerals
Because of this chemical interference, preparing your solution with distilled or deionized water is always the superior choice if you want to guarantee true high-level efficacy. Alkaline water with a pH above 8.0 slows down the formation of hypochlorous acid, which is the actual germ-killing engine of your mixture. If the chlorine cannot form this acid, your hard-fought 1000 ppm solution behaves more like a weak 400 ppm rinse. Have you actually tested the pH of your facility's tap water this quarter?
Why Hot Water Ruins Your Disinfectant Potency
And then there is the temptation to use scalding hot water under the false assumption that heat boosts cleaning power. The issue remains that heat rapidly destabilizes sodium hypochlorite, causing the active chlorine gas to evaporate directly into the air. Within minutes of mixing bleach with hot water, your high level disinfection 1000 ppm solution degrades into a useless pool of salty water. Always use cool, room-temperature water around 20 degrees Celsius to ensure the chemical bonds remain intact long enough to do their job.
Evaluating Bleach Alternatives for High-Level Disinfection
While sodium hypochlorite remains the undisputed, dirt-cheap king of global decontamination, modern facility managers are increasingly looking toward alternative chemistries. The classic chlorine mix ratio for a high level disinfection 1000 ppm is notoriously tough on equipment, prompting the adoption of less destructive options like accelerated hydrogen peroxide or peracetic acid. Experts disagree on whether these newer agents truly match the raw, broad-spectrum cost-efficiency of traditional bleach, but the operational trade-offs are worth examining.
Accelerated Hydrogen Peroxide Versus Chlorine
Accelerated hydrogen peroxide formulations typically require a 0.5% to 2% working concentration to achieve the same microbial kill rates that a 1000 ppm chlorine mixture guarantees. The primary advantage here is environmental safety; hydrogen peroxide breaks down cleanly into water and oxygen gas, leaving absolutely no toxic residues behind. Except that these proprietary formulations cost up to ten times more than a standard jug of industrial bleach. This massive price premium makes it a tough sell for cash-strapped public health clinics or high-volume veterinary hospitals that burn through dozens of gallons of disinfectant every single day.
Common Pitfalls and Volumetric Misconceptions
Math trips up even veteran infection control practitioners. The problem is that people confuse household splash-less variants with raw, unadulterated sodium hypochlorite. You cannot simply grab any bottle off a supermarket shelf and assume a generic dilution blueprint will safeguard your clinical environment. A high level disinfection 1000 ppm formulation demands rigorous precision, yet personnel routinely eyeball the measurements.
The "More is Better" Fallacy
Glancing at a murky bucket might tempt you to splash an extra glug of chemical. Stop right there. Escallating the potency does not accelerate microbial death; instead, it corrodes expensive diagnostic machinery and triggers respiratory distress among your staff. Why risk destroying a ten-thousand-dollar endoscope just because somebody felt lazy with a graduated cylinder? Over-concentration creates hazardous off-gassing. It is a toxic gamble that yields zero additional germicidal benefits.
Ignoring the Expiration Clock
Bleach degrades faster than most clinicians realize. Except that we rarely check the manufacture date stamped on the cardboard box. Once open, that jug loses its molecular punch within thirty days due to ambient temperature fluctuations and UV exposure. You might think you are deploying a robust germicide, but you are actually washing surfaces with inert, salty water. Testing the efficacy with chemical indicator strips is the only way to verify you have actually achieved the required 1000 ppm high-level disinfectant strength.
The Disastrous Pre-Cleaning Omission
Organic debris acts as a literal shield for pathogens. If blood, bioburden, or fecal matter blankets a surface, the chlorine ions aggressively oxidize those materials first, entirely exhausting their biocidal potential before reaching the underlying cellular matrix. Because of this rapid chemical neutralization, applying the solution directly to uncleaned spills defeats the entire purpose of your sanitation protocol. You must clean before you disinfect.
The Impact of Water Temperature and pH Dynamics
Let's be clear: the chemical architecture of chlorine is notoriously finicky. Most protocols completely ignore the thermal and chemical properties of the tap water used for mixing, which remains a massive blind spot in institutional sanitation. Mixing bleach to 1000 ppm chlorine in scalding hot water accelerates the decomposition of hyporous acid into inactive chlorates. As a result: your highly anticipated pathogen-killing solution turns impotent before it even touches the floor.
The Hypochlorous Acid Sweet Spot
Cold or lukewarm water is mandatory to stabilize the formulation. When you alter the pH of the water matrix, you shift the delicate equilibrium between hypochlorite ions and hypochlorous acid. The latter is a vastly superior germ-killer, boasting a penetration velocity nearly eighty times faster than its ionized sibling. If your local water supply is heavily alkaline, your high level disinfection 1000 ppm mix ratio will underperform dramatically unless the pH is monitored and maintained between 6.0 and 7.5. (We admit that tracking pH in a busy hospital utility closet is a logistical headache, but true high-level sterilization brooks no compromises).
Frequently Asked Questions
What is the shelf life of a 1000 ppm solution once mixed?
A freshly prepared batch maintains its stability for a maximum of 24 hours. Data from environmental hygiene studies indicates that chlorine concentration drops by up to 15% within a single day when stored in an open container at 22 degrees Celsius. Ultraviolet radiation accelerates this breakdown exponentially, converting active free chlorine into harmless but useless salt compounds. You must discard any leftover mixture at the end of every shift and prepare a clean batch to guarantee efficacy. Utilizing opaque, tightly sealed polyethylene bottles can minimize this degradation, yet the 24-hour expiration rule remains absolute across all standardized medical frameworks.
Can this concentration kill Clostridioides difficile spores?
No, standard household applications at this strength are insufficient for eradication. While a high level disinfection 1000 ppm baseline destroys vegetative bacteria, mycobacteria, and most enveloped viruses, it fails against stubborn bacterial endospores. Overcoming the rugged protein coat of C. diff requires a massive leap to 5000 ppm, which represents a 1:10 dilution of standard 5.25% commercial bleach. Clinical facilities must implement specific sporicidal agents rather than relying on this weaker formulation when menghadapi an active spore outbreak. Substituting one concentration for another out of convenience invites systemic contamination across your wards.
How does organic load affect the efficacy of the mix?
Heavy bioburden immediately deactivates the free available chlorine through rapid oxidation. When proteins or bodily fluids are present, the active chlorine molecules bind to these substances, creating chloramines and reducing the sanitizing power by up to 60% within the first two minutes of contact. This dramatic reduction means that an uncleaned surface can cause a 1000 ppm solution to plunge below the effective germicidal threshold almost instantly. For this reason, a two-step process involving an initial enzymatic detergent wash followed by the disinfectant application is non-negotiable. Skipping the preliminary wipe-down renders even the most precise chemical measurements completely useless.
An Uncompromising Paradigm on Bio-Security
We need to stop treating chemical reconstitution like a casual culinary recipe. The reality of infection control demands absolute adherence to molecular science, not rough estimations or hurried guesswork. Implementing a proper 1000 ppm high level sanitizing protocol represents the thin line between a safe clinical environment and a catastrophic outbreak of healthcare-associated infections. Yet institutions consistently cut corners by neglecting water quality, ignoring chemical degradation curves, and failing to educate frontline environmental service workers on the underlying chemistry. If your facility refuses to invest in precise volumetric dispensing systems and high-quality testing strips, you are merely performing the theater of cleanliness. True disinfection is an exact science that requires meticulous execution, unwavering vigilance, and a complete rejection of institutional complacency.