The Structural Reality: Decoding the Brain and the Arterial Bulge
To grasp why the brain reacts so dramatically in the long run, we have to look at what actually happens during the initial crisis. An aneurysm is fundamentally a structural failure—a weakening in the tunica media, the muscular middle layer of an artery wall, which causes a ballooning effect under the relentless pressure of systolic blood flow. When clinicians talk about what are the long-term effects of aneurysm surgery, they are fundamentally analyzing how the brain heals from both the initial arterial structural vulnerability and the trauma of the subsequent surgical intrusion. The thing is, the brain dislikes interference.
The Disruption of the Circle of Willis
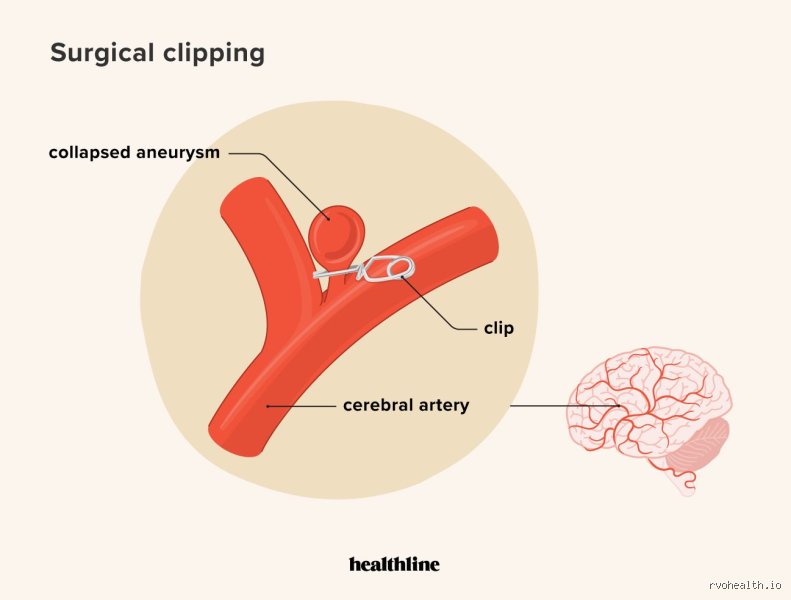
Most intracranial aneurysms develop within the Circle of Willis, the critical anastomotic ring of arteries at the base of the brain that ensures collateral circulation. When a surgeon places a titanium clip across the neck of an aneurysm—a procedure pioneered by Dr. Walter Dandy in 1937—or when an interventional neuroradiologist packs the space with platinum coils, the local hemodynamics alter instantly. Because the brain relies on micro-adjustments in pressure, this abrupt alteration can sometimes trigger localized ischemia or alter long-term perfusion patterns in adjacent tissues. We're far from it being a simple plumbing fix.
Ruptured vs. Unruptured Outcomes
Here is where it gets tricky, and frankly, where conventional wisdom often fails to paint the full picture. The long-term trajectory is radically different depending on whether the surgery was prophylactic or an emergency intervention following a subarachnoid hemorrhage (SAH). In unruptured cases, the long-term effects are largely a consequence of surgical access and minimal tissue retraction. But if a rupture occurred, the brain has already been exposed to neurotoxic blood breakdown products like hemosiderin, which causes chemical meningitis and triggers vasospasm. This distinction changes everything for the patient's future.
Neurological and Cognitive Evolution: The Hidden Tax on the Brain
Months after the incisions have healed at major centers like the Mayo Clinic or Johns Hopkins, patients often find themselves dealing with an invisible tax on their processing speed. Yet, their standard neurological exams might show perfect motor function. Why does this happen? Because the long-term effects of aneurysm surgery frequently manifest not as paralysis, but as subtle alterations in executive functioning, memory retrieval, and sustained attention.
[Image of brain aneurysm clipping surgery]The Chronic Fatigue Phenomenon
This isn't typical tiredness that a good night's sleep can fix. Neuro-fatigue is a profound, debilitating exhaustion resulting from the brain having to work twice as hard to route signals around old areas of surgical disruption or minor ischemic injury. And honestly, it's unclear exactly why some patients suffer from this for decades while others bounce back within a year—experts disagree on the precise mechanism, though many point to altered neurotransmitter pathways. A patient might manage a 30-minute grocery trip but then require four hours of silence in a dark room just to recalibrate. People don't think about this enough when evaluating surgical success.
Executive Function and Memory Faults
But the deficits can be even more specific, focusing on the frontal lobe networks that govern multitasking and emotional regulation. A study tracking 150 patients over five years might show that while their IQ scores remain stable, their ability to manage complex finances or tolerate chaotic environments is permanently degraded. Is it a direct result of the titanium clip resting against a microscopic branch of the anterior communicating artery, or is it a psychological scar from facing mortality? The answer is usually an intertwined combination of both factors.
The Psychological Landscape: PTSD and the Shadow of Recurrence
The human brain is not just a collection of wiring; it is the seat of identity. Consequently, the psychological long-term effects of aneurysm surgery are often the most difficult to manage because they are entirely internal. Many survivors walk through life feeling like a walking time bomb, even when their follow-up angiograms show a 99% occlusion rate of the treated lesion.
Post-Traumatic Stress and Vigilance
Every sudden headache becomes a potential catastrophe. This hyper-vigilance frequently crosses the line into clinical Post-Traumatic Stress Disorder (PTSD), a condition that a 2022 multi-center study found in up to 35% of SAH survivors during long-term follow-up. Except that instead of being triggered by external sounds or sights, these patients are triggered by their own internal bodily sensations. It is an exhausting way to live, which explains why psychological counseling must be viewed as a core component of long-term neurological rehabilitation rather than an optional afterthought.
The Burden on Social and Professional Spheres
Personality changes can alienate families who expect the patient to return "normal" once the physical scars fade. I have seen marriages fracture not because the patient couldn't walk, but because their emotional register became flat, or their impulse control eroded slightly after a complex basilar artery repair. It's an agonizing nuance that data points fail to fully capture.
Comparing Approaches: Clipping vs. Endovascular Coiling Long-Term Outcomes
The choice of surgical modality creates distinct long-term pathways that patients must navigate for the rest of their lives. The historic debate between open microvascular clipping and endovascular coiling isn't just about the recovery time in the first 30 days; it influences the entire next decade.
The Durability of the Open Clip
Open craniotomy for clipping is undeniably invasive, requiring the temporary removal of a bone flap and the retraction of brain tissue to place a mechanical clamp. But the long-term benefit? It is exceptionally durable. The recurrence rate for a completely clipped aneurysm is less than 2% over 10 years, meaning that once the long-term effects of aneurysm surgery from an open approach are stabilized, the risk of a future rupture from that specific site is practically eliminated.
The Coiling Paradigm and the Need for Surveillance
Endovascular coiling, or the deployment of flow-diverting stents like the Pipeline device, avoids opening the skull entirely by accessing the brain through the femoral or radial artery. It sounds perfect, right? Well, the issue remains that coils can compact over time under the relentless pounding of the pulse wave. Because of this risk of recanalization, endovascular patients face a lifetime of regular surveillance, including magnetic resonance angiograms (MRAs) or conventional digital subtraction angiography (DSA) at 1-year, 5-year, and 10-year intervals. As a result: these patients never truly leave the care of their neuroradiologist, introducing a chronic medicalization of their daily existence that open-surgery patients often escape.
Common mistakes and misconceptions about post-surgical recovery
The myth of the instantaneous reset
You leave the operating room, the titanium clip is secure, and you assume the ordeal is instantly over. Except that the brain does not operate on the timeline of a surgical calendar. Many patients confuse surgical success with immediate biological restoration. They expect their pre-pathology energy levels to return the moment anesthesia fades. This misunderstanding triggers immense psychological distress when persistent fatigue or mild cognitive stutters linger for six months or more. Neuroplasticity demands chronological runway. Healing is a grueling, non-linear marathon, not an electrical switch you just flip back to the on position.
Equating structural stability with functional perfection
Let's be clear: a perfectly occluded sac does not automatically mean flawless neurological output. Radiologists love a pristine post-operative angiogram showing zero residual blood flow. Neurosurgeons celebrate structural victory, which is entirely fair given the stakes. However, the surrounding brain tissue often suffers subtle ischemic or inflammatory insults during the microdissection phase. Why do you still struggle with multitasking if the repair was flawless? Because macroscopic architecture and microscopic pathways are two entirely different realms. A successful operation prevents a catastrophic hemorrhage, yet it occasionally leaves minor, localized collateral disruptions that require targeted cognitive rehabilitation.
Assuming endovascular coils are temporary fixtures
A bizarre but frequent assumption among patients undergoing endovascular treatment is that platinum coils or flow-diverting stents will eventually need replacement. This is completely false. These biomedical implants are engineered to remain inside your intracranial circulation forever. Over time, your body actually endothelializes the device, meaning a natural layer of cellular tissue grows over the metallic matrix to permanently seal it off. You will not need a tune-up or a hardware swap in ten years.
The silent neurovascular tax: What they don't tell you
The burden of hyper-vigilance and localized headaches
There is a hidden cost to surviving a neurovascular intervention that rarely makes it into clinical brochures. We call it the psychological echo of the aneurysm. Every minor tension headache or transient dizzy spell suddenly feels like an impending rupture. This persistent hyper-vigilance induces chronic sympathetic nervous system arousal, which ironically elevates your blood pressure. And what is the primary threat to your long-term vascular integrity? Sustained hypertension. It is a vicious, self-fulfilling loop. Furthermore, localized discomfort near the craniotomy site can persist for years due to severed cutaneous nerves or temporal muscle atrophy. It is an annoying, benign nuisance, but one that regularly panics patients who have not been properly warned about the long-term effects of aneurysm surgery.
The necessity of lifetime surveillance
Can you simply forget about your brain once you hit the five-year milestone? Hardly. While the risk of a recurrence at the treated site drops drastically after complete surgical clipping, the systemic vulnerability remains. Your genetics did not change on the operating table. The issue remains that patients who have developed one lesion possess approximately a 10% to 15% chance of forming an entirely new, de novo vascular anomaly elsewhere in the circle of Willis over their lifetime. Which explains why your medical team will insist on non-invasive imaging every few years. It is a minor inconvenience, but absolute vigilance is your only real shield against future cerebrovascular surprises.
Frequently Asked Questions
What is the statistical likelihood of experiencing cognitive deficits after clipping versus coiling?
Data from long-term observational cohorts indicate that approximately 30% of patients undergoing open craniotomy for surgical clipping report measurable deficits in executive functioning or memory at the one-year mark. Conversely, endovascular coiling cohorts demonstrate a slightly lower initial cognitive friction rate of roughly 18% due to the avoidance of direct brain retraction. However, these statistical variances largely equalize by the five-year mark as the brain undergoes delayed axonal remodeling. The baseline severity of the initial presentation, specifically whether the lesion had ruptured before intervention, remains the true mathematical predictor of your ultimate cognitive trajectory. Age and pre-existing small vessel ischemic disease further compound these objective neurological outcomes over time.
How long must I wait before safely returning to high-intensity cardiovascular exercise or heavy lifting?
Most neurovascular institutions enforce a strict restriction on heavy lifting exceeding twenty pounds for at least six to eight weeks following any intracranial intervention. Your systemic blood pressure spikes dramatically during the Valsalva maneuver, which places immense, dangerous shear stress on healing arterial walls. For endovascular procedures, the femoral or radial access site dictates the immediate timeline, requiring absolute rest for several days to prevent hematoma formation. Once follow-up digital subtraction angiography confirms stable occlusion at six months, most patients receive clearance for vigorous cardiovascular activities. But you must commit to an incremental pacing strategy rather than attempting to smash your old personal records immediately.
Will the titanium clips or platinum coils trigger airport metal detectors or restrict future MRI scans?
Modern intracranial implants are constructed from medical-grade titanium alloys and platinum, which are entirely non-ferromagnetic materials. As a result: you will not set off standard airport security scanners or transport hub metal detectors when going through checkpoints. These advanced materials are also completely safe for subsequent magnetic resonance imaging, typically up to standard 3-Tesla field strengths. You must, however, always carry your specific implant identification card to provide the radiology technicians with exact manufacturing specifications. The only real imaging drawback is the localized artifact or blind spot the metal creates on the scan, which occasionally obscures the tissue immediately adjacent to the repaired vessel.
A definitive perspective on post-surgical neurovascular life
Surviving an intracranial intervention changes the fundamental chemistry of your existence, whether you want it to or not. We must stop treating the long-term effects of aneurysm surgery as a simple checklist of physical healing milestones. The true journey is deeply psychological and systemic, requiring a radical acceptance of your own vascular vulnerability. Do you want to live in perpetual fear of a secondary rupture, or will you use this clinical second chance to aggressively optimize your cardiovascular health? The data shows that lifestyle modifications, particularly meticulous blood pressure management and the permanent cessation of tobacco use, alter your survival metrics far more than the initial choice between a catheter or a scalpel. You are not a broken vessel waiting to leak again; you are a reinforced biomechanical marvel. Take ownership of your recovery, accept the subtle cognitive shifts as the price of survival, and move forward with absolute intent.