The Ticking Clock Inside the Cranium: Defining the Vascular Threat
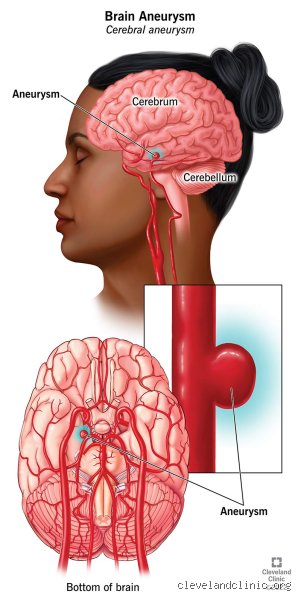
To understand the lasting wreckage, we must first look at what we are actually dealing with here. A cerebral aneurysm is essentially a weakened, bulging spot in the wall of an artery within the brain, often resembling a tiny berry hanging from a stem. For years, these malformations can sit silently in the Circle of Willis—the network of arteries at the base of the brain—without causing a single symptom. People walk around, drink coffee, and go to work entirely oblivious to the structural vulnerability inside their heads. The thing is, when that structural weakness gives way, it triggers a subarachnoid hemorrhage, a catastrophic type of stroke where blood floods the space surrounding the brain.
The Anatomy of a Rupture
When blood escapes under high pressure, it does not just sit there. It actively destroys. The initial surge damages surrounding neural tissue within seconds, which explains why survivors often describe the event as the worst headache of their life. But the immediate trauma is only the first wave. The real trouble starts days later. Neurologists at the Mayo Clinic have frequently documented that the presence of free-flowing blood causes intense irritation to neighboring blood vessels. This leads to vasospasm, a condition where arteries narrow violently, choking off the oxygen supply to healthy parts of the brain and causing secondary ischemic strokes. That changes everything for the patient's prognosis.
The Silent Counterpart: Unruptured Anomalies
But what about the ones that do not burst? This is where it gets tricky. An unruptured aneurysm that is discovered incidentally during an MRI for an unrelated issue—like chronic migraines or a minor concussion—carries its own psychological weight. Even without a bleed, a large anomaly can compress cranial nerves, leading to localized problems like a drooping eyelid or double vision. Yet, the most pervasive long-term effect here is often not physical at all. How do you live a normal life knowing a blood vessel in your head might fail? The chronic anxiety resulting from this medical sword of Damocles is a profound, lingering consequence that clinical trials frequently fail to measure accurately.
Neurocognitive Fallout: Why Life Looks Different After a Brain Crisis
Survival is just the starting line, not the finish. Ask anyone who walked out of a neurological ICU after an endovascular coiling or a surgical clipping procedure, and they will tell you that the person who returned home was not exactly the person who left. The long-term effects of a ruptured aneurysm regularly manifest as a frustrating haze of cognitive challenges. Memory retrieval becomes sluggish. Executive functioning—the brain's ability to plan, focus, and multitask—essentially glitches out when faced with complex situations. Honestly, it's unclear why some areas recover beautifully while others remain permanently derailed, as experts disagree on the exact threshold of irreversible ischemic damage during the acute phase.
The Exhaustion That Sleep Cannot Fix
We are far from a complete understanding of post-aneurysm fatigue, which is nothing like normal tiredness. It is an overwhelming, cellular exhaustion that zeroes out a person's energy reserves after simple tasks like reading a grocery list or holding a conversation. Neurosurgeons hypothesize that this occurs because the brain has to work twice as hard to route signals around damaged neural pathways. Imagine trying to navigate a major metropolitan area during rush hour after a massive earthquake has cracked the main highways—you might eventually reach your destination, but the detour consumes massive amounts of fuel. Because of this, returning to a demanding forty-hour work week becomes an insurmountable wall for many survivors.
Emotional Rewiring and Personality Shifts
And then there is the emotional volatility. Family members often notice a distinct shift in temperament. A previously calm, patient individual might suddenly struggle with intense irritability, sudden bouts of depression, or an inability to regulate their anxiety. Is this a direct result of physical tissue damage in the frontal lobe, or is it the psychological trauma of surviving a near-death experience? It is almost certainly a complex cocktail of both. In a notable 2022 observational study conducted in Edinburgh, researchers tracked eighty-five subarachnoid hemorrhage survivors and found that over forty percent met the clinical criteria for Post-Traumatic Stress Disorder years after their physical wounds had healed.
The Secondary Complications That Refuse to Leave
The long-term effects are not confined to the abstract realms of mood and memory; they frequently manifest as concrete physical ailments. When an aneurysm ruptures, the resulting debris can block the natural flow and drainage of cerebrospinal fluid. This blockage leads to hydrocephalus, a buildup of fluid that exerts dangerous pressure on the brain. While some patients receive a temporary drain in the hospital, others require a permanent ventriculoperitoneal shunt to bypass the obstruction. Living with a shunt means accepting a lifelong risk of mechanical failure or infection, turning a past crisis into a permanent management routine.
The Electrical Storm: Post-Hemorrhagic Epilepsy
Another lingering threat is the development of seizures. The scarring left behind by iron deposits in the blood acts like an irregular electrical ground in a house's wiring system. This structural scarring can spark abnormal electrical activity, resulting in epilepsy months or even years after the initial event. Survivors must often take potent anticonvulsant medications indefinitely. These drugs carry their own baggage, including chronic drowsiness and a distinct mental fog that further complicates the recovery process. People don't think about this enough when they look at a survivor who appears physically whole from the outside.
Contrasting Recovery Paths: Coiling Versus Clipping
How the medical team fixes the vascular defect in the acute stage plays a massive role in shaping the long-term effects a patient will face. For decades, the gold standard was surgical clipping, a highly invasive craniotomy where a surgeon cuts through the skull to place a tiny metal clip across the neck of the bulge. More recently, endovascular coiling has dominated the field. This less invasive technique involves guiding a catheter up through the femoral artery in the groin all the way into the brain to pack the aneurysm with platinum wires, inducing clotting from the inside out.
The Trade-offs of Modern Intervention
Yet, the easier path into the brain does not always guarantee a smoother decade ahead. While endovascular coiling boasts a much shorter immediate recovery time and fewer early complications, the long-term recurrence rates are notably higher compared to surgical clipping. Data from the landmark International Subarachnoid Aneurysm Trial revealed that coiled anomalies occasionally require follow-up monitoring and additional touch-up procedures because the coils can compact over time under the relentless pounding of arterial blood pressure. As a result: a patient who underwent coiling may face a lifetime of periodic angiograms and the recurring anxiety that accompanies every single scan, whereas a clipped patient typically enjoys a more definitive, albeit harder-earned, structural cure. Except that the physical trauma of opening the skull during a craniotomy sometimes leaves localized muscle wasting, jaw pain, or chronic headaches that never truly disappear.