The Hidden Anatomy: What Does a 5mm Aneurysm Actually Look Like?
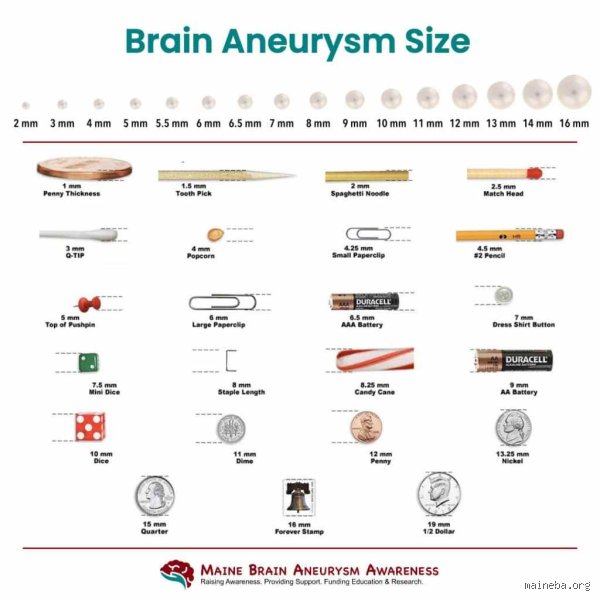
Let us strip away the clinical sterility for a second. We are talking about a blister on an artery, a structural failure where the muscular layer of a blood vessel gives way under the relentless thumping of your pulse. When a radiologist in Boston or London measures this bulge at five millimeters, they are looking at something roughly the size of a single peppercorn. Sounds tiny, right? Except that this peppercorn is nestled directly inside the subarachnoid space of your brain, sitting alongside fragile neural pathways where even a microscopic leak alters everything in a heartbeat.
The Mechanics of the Intracranial Bulge
The thing is, size isn't the only metric that dictates danger. Most of these lesions are saccular—often called berry aneurysms—which means they protrude like a tiny dome from the side of a vascular fork. But why do they form there? Blood flow in the Circle of Willis, the main arterial ring supplying the brain, is highly turbulent. If your genetics handed you thinner arterial walls, or if decades of unrecognized hypertension have been hammering those vessel bifurcations, the tissue eventually stretches out. I firmly believe that treating these solely as "geometric anomalies" is a fundamental mistake made by old-school medicine; they are dynamic, living structural failures that react to every spike in your adrenaline.
Symptoms That Arrive by Accident
Here is where it gets tricky: an unruptured 5mm aneurysm almost never causes physical symptoms on its own. It is simply too small to compress the surrounding cranial nerves or displace brain tissue, which explains why the vast majority are discovered as incidentalomas during an MRI for an unrelated concussion or persistent vertigo. But when symptoms do manifest—perhaps a subtle, localized ache behind the left eye or a sudden patch of double vision—it usually implies the aneurysm is actively changing shape or exerting pressure on the third cranial nerve. If that happens, the clinical conversation shifts instantly from casual monitoring to scheduling an operating room.
Predicting the Unpredictable: Rupture Risk Assessment for Small Lesions
For decades, neurosurgeons operated under the assumption that any structural defect in a cerebral artery was a medical emergency requiring immediate, aggressive intervention. That changed dramatically after the publication of the International Study of Unruptured Intracranial Aneurysms (ISUIA), a landmark trial that tracked thousands of patients across North America and Europe to see who actually suffered a subarachnoid hemorrhage. The data sent shockwaves through the neurological community, revealing that unruptured lesions smaller than 7mm had an annual rupture rate of nearly 0% if they were located in the anterior circulation.
Decoding the PHASES Score and Statistical Realities
Today, physicians do not just guess; they utilize the PHASES score, a sophisticated predictive model based on pooled data from international cohorts. This algorithm weighs your geographic ancestry (with Japanese and Finnish populations carrying significantly higher baseline risks), your age, whether you have a history of subarachnoid hemorrhage from a different vessel, and the exact physical location of the bulge. If your 5mm lesion is located in the posterior communicating artery or the basilar artery, its threat level jumps significantly compared to an identical 5mm bulge on the internal carotid artery. It is a game of probability where a single point shift alters your entire management plan.
The Lifestyle Multipliers That Change Everything
Statistics are comforting until you realize they apply to populations, not to the unique individual sitting in a cold examination room. If you smoke a pack of cigarettes a day, that beautifully low 0.5% annual rupture risk statistic becomes completely irrelevant. Chronic nicotine exposure actively degrades the collagen matrix within the arterial wall, turning a stable, thick-walled pouch into a fragile, transluscent membrane. Combine smoking with uncontrolled systemic hypertension, or a history of heavy binge drinking on weekends, and you have created the perfect storm for structural failure regardless of what the millimeter measurement says on your chart.
The Geometric Nuances: Why Size is a Deceptive Metric
People don't think about this enough: a sphere is a very different beast than a irregular, bumpy sac with a narrow neck. When a neuroradiologist reviews a 3D CT Angiography (CTA) scan, they are looking far beyond the absolute diameter. A 5mm aneurysm that is perfectly smooth and round distributes wall shear stress evenly across its surface, making it remarkably stable over long periods. But if that same 5mm lesion features a tiny, secondary bleb protruding from its apex—what doctors call a daughter sac—the physics change completely because that micro-bud represents a localized zone of extreme tissue thinning.
The Critical Importance of Aspect Ratio
Where it gets truly dangerous is when the aspect ratio—the relationship between the depth of the aneurysm dome and the width of the arterial neck—is highly skewed. If you have a narrow neck and a long, elongated dome, the blood gets trapped inside the pouch, swirling under high pressure and creating intense localized friction against the fundus. Neurological centers in places like the Mayo Clinic have demonstrated that an aspect ratio greater than 1.6 is an independent predictor of rupture, even if the overall size remains firmly in the "small" category. Honestly, it's unclear why some small lesions possess these aggressive geometries while others remain flat, but the shape dictates the survival of the tissue.
Comparing Diagnostic Tools: MRA versus CTA versus DSA
You cannot manage what you cannot see with absolute precision. When an initial screening scan hints at a vascular abnormality, choosing the right follow-up imaging modality becomes a matter of supreme importance because a variance of just one millimeter can completely alter your treatment trajectory.
Magnetic Resonance Angiography (MRA) and Its Limits
An MRA is the favorite tool for long-term surveillance because it requires zero radiation and, in many cases, does not even need an intravenous contrast injection. It uses the natural movement of your blood to construct a digital map of your vasculature. Yet, for all its convenience, standard 1.5-Tesla or even 3-Tesla MRAs can suffer from significant artifact blurring when looking at things under 5mm, occasionally creating false positives or overestimating the true size of the neck. We are far from a world where an MRA alone is enough to plan a complex endovascular procedure.
The Gold Standard: Digital Subtraction Angiography (DSA)
When a definitive answer is mandatory, doctors turn to Digital Subtraction Angiography (DSA), an invasive procedure performed in a specialized cath lab. A neurointerventionalist inserts a thin catheter through your groin or radial artery, threading it all the way up into the vessels of your neck before injecting a contrast dye while taking rapid-fire X-ray movies. By digitally subtracting the images of your skull bones, they are left with an incredibly crisp, high-resolution view of the moving blood. It carries a tiny risk of causing a stroke—roughly 0.5% in experienced hands—but it provides the absolute truth regarding wall irregularities and flow dynamics that non-invasive scans simply miss.