The Hidden Reality of a Silent Vascular Balloon
Imagine a tiny, weakened patch on an inner tube. That is the reality of a cerebral aneurysm. Blood rushes through the brain's arterial network constantly—beating roughly 100,000 times a day—and over decades, this relentless hydrostatic pressure can cause a focal structural failure. Honestly, it's unclear precisely when or why certain walls give way while others hold firm for eighty years. It is a biological lottery.
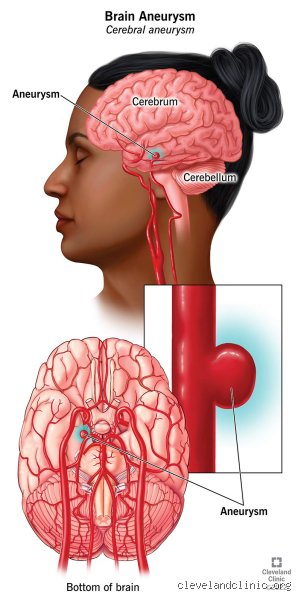
The Architecture of the Intracranial Bulge
Neurosurgeons at the Mayo Clinic usually categorize these lesions into two structural shapes: saccular and fusiform. Saccular variants, affectionately dubbed "berry" aneurysms by generations of medical students because of their distinct stem-and-dome silhouette, account for the overwhelming majority of cases. They sprout quietly, most frequently at the bifurcations of the Circle of Willis, which is the arterial ring nestled deep at the base of your skull. Fusiform aneurysms are different, appearing as an asymmetrical, elongated widening of the entire vessel wall. And because they lack a distinct neck, repairing them is an absolute logistical nightmare for an endovascular specialist.
Prevalence and the Accidental Patient
Here is a piece of data that turns conventional wisdom completely on its head: approximately 1 in 50 people in the United States currently has an unruptured brain aneurysm ticking away inside their head without a single clue. That translates to roughly 6.5 million Americans going about their grocery shopping, driving to work, and playing tennis with a vascular anomaly. Most of these individuals will eventually pass away from entirely unrelated causes—old age, heart disease, or perhaps a rogue distracted driver in Chicago—never realizing their brain harbored a structural defect. The thing is, we are diagnosing more of them than ever before simply because of the sheer ubiquity of modern neuroimaging. When a neurologist orders an MRI for an everyday tension headache or a minor bout of vertigo following a slip on the ice, they frequently stumble upon an incidentaloma—the medical jargon for an unexpected, accidental finding that changes everything for the patient overnight.
Deciphering the Rupture Equation and Statistical Realities
The core struggle for any patient diagnosed with this condition centers on a paradox of numbers. How do we balance the terrifying prospect of a subarachnoid hemorrhage against the inherent risks of invasive brain surgery? We are far from a definitive, one-size-fits-all crystal ball, but large-scale clinical trials have provided a roadmap.
The UCAS and ISUIA Studies That Changed the Game
For decades, physicians operated under a fog of guesswork until the International Study of Unruptured Intracranial Aneurysms (ISUIA) and the Unruptured Cerebral Aneurysm Study (UCAS) in Japan provided hard data. The ISUIA data shook the neurological community by demonstrating that aneurysms measuring less than 7 millimeters in the anterior circulation of the brain have an annual rupture rate of virtually zero percent. Zero! Let that sink in if you are currently panicking over a 3mm finding. But where it gets tricky is when that bulge crosses the critical threshold into the territory of large or giant aneurysms. For a lesion exceeding 25 millimeters, the five-year cumulative rupture rate skyrockets to an alarming 40 percent. Why such a drastic leap? Because fluid dynamics inside a larger dome become incredibly turbulent, creating localized stress zones that rapidly degrade the thinning collagen matrix of the vessel wall.
Location as a Hidden Determinant of Lifespan
An aneurysm's physical address within your cranium dictates its behavior just as much as its size. Lesions nesting in the posterior circulation—specifically the basilar artery or the vertebral arteries at the back of the brain—carry a significantly higher baseline threat level than those situated in the anterior communicating artery at the front. The issue remains that the posterior fossa is a cramped, unforgiving neighborhood where even a micro-leak can cause devastating pressure on the brainstem. People don't think about this enough: a 5mm bubble in the back of the head might demand immediate endovascular coiling, while an identical 5mm bubble near the ophthalmic artery at the front might safely be left alone, monitored via annual magnetic resonance angiograms for the next thirty years without a single millimeter of growth.
The Biological Clock: Age, Genetics, and Natural History
If you are diagnosed at age thirty, the lifetime risk calculation looks radically different than if a radiologist spots a bulge in your seventy-five-year-old grandmother. It is a game of cumulative exposure to the laws of physics and human biology.
The Long-Term Outlook for Younger Patients
A thirty-year-old patient with an unruptured aneurysm faces a sixty-year horizon of potential risk, meaning that even a low annual rupture rate of 0.5 percent compounds over time into a significant statistical probability. Yet, the systemic health of a younger person's vasculature provides a robust defense mechanism. Their arterial walls possess an elasticity that senior vessels have long since lost through the natural processes of cellular senescence. Except that youth also brings lifestyle variables that can destabilize a previously benign lesion. Sudden, extreme spikes in blood pressure from heavy weightlifting or intense psychological stress can, in rare instances, stress the aneurysm wall. But can you live to be ninety with it? Absolutely, provided the structural environment remains stable and you actively manage your systemic vascular health.
Symptomatic Versus Asymptomatic Presentation: The Critical Divide
We must draw a sharp, uncompromising line between an aneurysm that is completely silent and one that is beginning to make its presence known to the surrounding brain tissue. This distinction is where clinical nuance becomes a matter of life and death.
When the Silent Bulge Starts to Speak
An asymptomatic aneurysm is a passive occupant; a symptomatic unruptured aneurysm is an active threat to your longevity. When a vascular bubble expands to the point where it physically impinges upon adjacent cranial nerves, the clock begins to tick loudly. The classic presentation involves a sudden, unexplained palsy of the third cranial nerve, which manifests as a drooping eyelid (ptosis) and double vision where one eye looks down and out. This neurological deficit usually indicates that an aneurysm located at the junction of the internal carotid and posterior communicating arteries is undergoing acute expansion—a structural stretching that serves as an emergency warning shot. If left unaddressed, these symptomatic lesions have an incredibly high propensity to rupture within days or weeks, completely obliterating any hopes of a normal natural lifespan. Hence, symptomatic status instantly transforms a wait-and-see monitoring protocol into an urgent surgical mandate, regardless of whether the lesion measures 3mm or 20mm.
Common mistakes and dangerous misconceptions
The "ticking time bomb" psychological trap
Many patients diagnosed with this vascular anomaly immediately adopt a defeatist mindset, assuming that a rupture is imminent and guaranteed. This is a profound misunderstanding of the actual pathology. The reality is that a vast majority of these vascular bulges remain entirely quiescent throughout a person's natural life. How long can you live with an unruptured aneurysm? Often, you can live for decades without the lesion ever changing or causing neurological deficits. By obsessing over a worst-case scenario, patients frequently experience debilitating anxiety that actively degrades their quality of life, which explains why psychological support is just as vital as radiological monitoring.
Assuming all aneurysms require immediate surgical intervention
There is a prevailing myth that finding a bulge in a brain artery means you must head straight to the operating room. Let's be clear: the risks associated with prophylactic neurosurgery—whether endovascular coiling or open microsurgical clipping—can sometimes outweigh the natural history risk of the lesion itself. Data from the landmark International Study of Unruptured Intracranial Aneurysms (ISUIA) demonstrated that small anterior circulation aneurysms measuring under 7 millimeters in patients with no history of subarachnoid hemorrhage have a five-year rupture rate of effectively zero percent. Imaging technology has advanced significantly, meaning we catch these incidental findings more frequently now. Rushing into an invasive procedure for a tiny, stable lesion is often a miscalculation of risk.
The confusion between size and stability
Another frequent error is focusing exclusively on the diameter of the sac while ignoring its morphology. While a larger volume certainly elevates danger thresholds, irregular shapes, dynamic changes over time, and asymmetry or daughter sacs pose immense threats even in smaller lesions. If you believe a 5-millimeter bulge is universally safe, you are mistaken. Location matters immensely; for instance, lesions situated on the posterior communicating artery carry a disproportionately higher threat profile than those on the middle cerebral artery.
The hidden impact of systemic hemodynamic stress
Why your blood pressure variability matters more than the mean
Neurologists often preach about keeping blood pressure low, yet they rarely explain the nuance of hemodynamic spikes. It is not just your average daily numbers that dictate the structural integrity of the weakened arterial wall, but rather the sudden, violent surges in transmural pressure. Activities that induce the Valsalva maneuver—such as heavy weightlifting, severe coughing fits, or intense bouts of anger—can cause acute spikes where systolic pressure briefly exceeds 200 mmHg. This acute stress can compromise the thin collagen layer of the dome. If you want to know how long can you live with an unruptured aneurysm, the answer depends largely on how well you avoid these radical hemodynamic rollercoasters.
The silent destruction caused by ongoing nicotine exposure
Smoking is not just a general health hazard; it actively degrades the extracellular matrix of the blood vessel. Nicotine triggers the upregulation of matrix metalloproteinases, which are enzymes that literally chew away at the structural scaffolding of your cerebral arteries. Except that many patients think cutting back is enough. It is not. Total cessation is mandatory because active smokers face a threefold increase in rupture risk compared to non-smokers, making lifestyle modifications far more impactful than merely sitting around waiting for your next annual magnetic resonance angiogram.
Frequently Asked Questions
Can you live a normal life with an unruptured brain aneurysm?
Yes, thousands of individuals navigate their entire lives normally without ever knowing a vascular irregularity exists in their cranium. Autopsy data reveals that approximately 1 in 50 people harbor an asymptomatic intracranial aneurysm, yet only a tiny fraction of these cases experience a catastrophic subarachnoid hemorrhage. You can work, exercise moderately, and grow old, provided you manage your cardiovascular health diligently. The issue remains that you must modify extreme behaviors, meaning competitive powerlifting or scuba diving might require reevaluation. In short, normalcy is entirely achievable if you swap panic for structured, professional medical surveillance.
What are the specific warning signs that an unruptured aneurysm is growing?
Most stable vascular bulges produce absolutely no symptoms, but a growing sac can begin compressing adjacent cranial nerves and brain tissue. You might experience localized headaches, blurred or double vision, or a dilated pupil if the lesion sits near the oculomotor nerve. Because these signs mimic benign conditions, they are frequently dismissed until a crisis occurs. (A sudden, severe "thunderclap" headache is not a warning sign of growth, but rather an indicator that a rupture has already taken place). If you notice progressive, unexplained neurological deficits on one side of your face, you need an immediate imaging update.
How long can you live with an unruptured aneurysm if it is left untreated?
Statistically, an individual can harbor a stable, small vascular bulge for thirty, forty, or even fifty years without it ever impacting their lifespan or neurological function. A 2012 study published in The Lancet Neurology established that for small, asymptomatic lesions, the annualized risk of rupture is often less than one percent per year. Consequently, a 65-year-old patient diagnosed with a 4-millimeter internal carotid artery lesion will likely die of old age or unrelated cardiac issues long before the aneurysm poses a tangible threat. Your longevity with an untreated lesion is directly tied to its specific anatomical location, its initial size, and your genetic predisposition to vascular weakness.
An honest paradigm shift in vascular preservation
We need to stop treating an incidental vascular diagnosis as an automatic death sentence or a mandatory invitation to the operating table. The aggressive marketing of intervention options often overshadows the profound power of conservative medical management and lifestyle transformation. Forcing an invasive catheter or a titanium clip into a stable, quiet brain artery to satisfy a patient's anxiety is bad medicine. As a result: we must demand a higher standard of customized care that prioritizes rigorous blood pressure control, absolute smoking cessation, and precise serial imaging over premature surgical heroics. Can we predict every single rupture with absolute certainty? No, our predictive models have clear limits, and anyone claiming perfect foresight is being dishonest. But by focusing our clinical energy on modifiable risk factors rather than just the structural geometry of the vessel, we can safely guide patients toward a long, full life. True medical mastery lies in knowing when to intervene, but more importantly, having the courage to watch, wait, and protect.