Finding out there is a ticking time bomb—or what feels like one—inside your skull changes everything in a fraction of a second. You went into the clinic for a stubborn migraine or a minor concussion from a fender bender on I-95, and you walked out with a radiological report that feels like a psychological anchor. It is terrifying. But here is where we need to inject some cold, hard reality into the panic: the annual rupture rate for small, asymptomatic aneurysms is often less than 1% per year. I believe the medical community sometimes fails patients by delivering this diagnosis with the solemnity of an obituary rather than the pragmatic framing of a manageable anatomical quirk. We need to look at the data, not the fear.
What Exactly Happens Inside the Skull When an Aneurysm Forms?
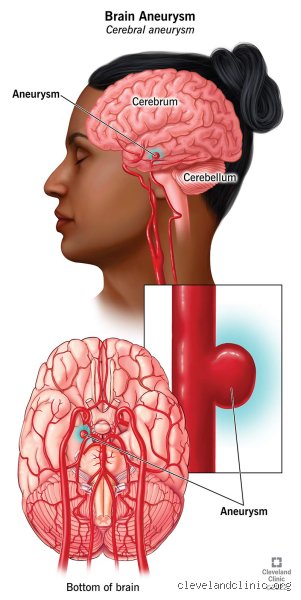
To understand why these vascular anomalies behave the way they do, we have to look at the plumbing. Your brain demands a massive, uninterrupted blood supply, which is delivered through a network of arteries that meet at the base of the brain in a structural ring called the Circle of Willis. Think of it as a high-pressure highway intersection where the asphalt is constantly taking a pounding from torrential traffic.
The Anatomy of a Weakened Vascular Wall
An aneurysm develops when a specific weak spot in the arterial wall yields to the relentless, pounding force of systolic blood pressure, causing the vessel to balloon outward. It is a structural failure of the tunica media, the muscular middle layer of the artery. As blood rushes into this newly formed pouch, the wall thins out even further, mimicking a overinflated rubber balloon. Why does this happen to some people and not others? The thing is, genetics play a massive role, particularly if you have a first-degree relative who suffered a subarachnoid hemorrhage, but acquired lifestyle factors are what usually push the vascular tissue past its breaking point over decades of wear and tear.
Saccular Versus Fusiform: Not All Bulges Are Created Equal
Neurosurgeons broadly categorize these lesions into distinct structural types, and the shape dictates your entire prognosis. The most common variety, comprising about 90% of intracranial aneurysms, is the saccular—or "berry"—aneurysm, which protrudes from a distinct neck at an arterial bifurcation. Then you have fusiform aneurysms, which are entirely different beasts because they involve the widening of the entire circumference of the blood vessel over a longer segment. Where it gets tricky is that fusiform types rarely rupture out of nowhere; instead, they tend to cause trouble by clotting or compressing nearby brain tissue, which completely flips the treatment strategy on its head.
Predicting the Unpredictable: How Doctors Calculate Your Rupture Risk
This is where the conventional wisdom of the internet gets it wrong, because you cannot treat every aneurysm with a one-size-fits-all panic meter. When a patient sits down at a major neurological hub like the Mayo Clinic in Rochester, the specialists do not just guess; they rely on massive historical data sets to mathematically weigh the probability of a bleed against the very real risks of brain surgery.
The PHASES Score and the Power of Millimeters
Neurologists rely heavily on the PHASES score, a validated prognostic tool established after analyzing data from thousands of patients across international cohorts. This system scores risk based on six key variables: population demographics, hypertension, age, size of the aneurysm, earlier subarachnoid hemorrhage from another aneurysm, and the specific site of the lesion. Size is arguably the heaviest anchor in this equation. Data shows that an aneurysm measuring less than 7 millimeters in the anterior circulation of a patient without a history of ruptures has an incredibly microscopic chance of leaking. But wait, if small ones are so safe, why do neurosurgeons still occasionally operate on them? Because location changes the math completely.
The Geography of the Circle of Willis
Location is everything. An aneurysm nestled quietly in the internal carotid artery presents a radically different threat level than one sitting on the posterior communicating artery or the basilar tip. The posterior circulation vessels handle turbulent, high-velocity blood flow coming straight from the brainstem. If a 5-millimeter bulge is detected in the back of the head, clinicians worry far more than if that same 5-millimeter bulge were sitting in the anterior communicating artery up front. But honestly, it's unclear why certain small posterior lesions remain stable for forty years while others give way, which explains why the medical community remains locked in fierce debates during grand rounds every single week.
The Asymptomatic Reality: Why Most People Never Feel a Thing
The vast majority of people living with an unruptured brain aneurysm have absolutely zero physical symptoms. None. They are out mowing the lawn, running marathons, or sitting in corporate boardrooms completely oblivious to the fact that their cerebral arteries have a structural deviation. Except that sometimes, as an aneurysm grows, it begins to crowd its neighbors.
The Warning Signs of a Mass Effect
When an aneurysm expands to a significant size—usually crossing into the "large" territory above 10 millimeters—it can exert what neurologists call a mass effect on surrounding brain tissue and cranial nerves. This is not a rupture, mind you, but a mechanical crowding. A classic manifestation is the sudden development of a drooping eyelid or a dilated, unresponsive pupil, which happens because an aneurysm on the posterior communicating artery is physically pressing against the third cranial nerve. If you experience sudden, unexplained double vision or localized pain behind one eye, that changes everything, because it suggests the aneurysm is actively changing shape or stretching the nerve fibers. People don't think about this enough: a symptomatic unruptured aneurysm is an absolute medical emergency that requires immediate admission, even if it hasn't spilled a single drop of blood yet.
To Watch or to Weave: Comparing Active Surveillance and Proactive Intervention
Once the initial shock wears off, you face a massive crossroads: do you leave the aneurysm alone and watch it, or do you let a physician thread a catheter into your brain to fix it? It is a profound psychological trade-off between the systemic risks of an invasive procedure and the mental burden of knowing you are carrying a physical vulnerability.
The Conservative Route: Watchful Waiting Under the Scanner
For millions, the wisest choice is active surveillance. This means you return to the imaging center every 6 to 12 months for a high-resolution Magnetic Resonance Angiogram (MRA) or a Computed Tomography Angiography (CTA) to check for any structural evolution. If the lesion remains completely static over a 24-month period, the monitoring intervals often stretch out to every two or three years. The issue remains, however, that living between scans can induce a severe form of psychological paralysis. Can you safely lift heavy weights? Is it okay to fly on a commercial airliner to London? Doctors often give vague answers because concrete data on transactional blood pressure spikes is sparse, yet the consensus remains that maintaining an active, low-stress life is far better for your blood vessels than rotting on a couch out of sheer terror.
The Proactive Alternative: When the Risk Math Favors Surgery
Conversely, when the PHASES score creeps into dangerous territory or a patient is young and facing fifty more years of cumulative exposure, watchful waiting loses its luster. Intervention becomes the logical path forward. We are far from the days when open-skull craniotomies were the sole option for every patient; the evolution of endovascular neurosurgery over the last two decades has completely revolutionized the field. But choosing surgery is not a casual decision, because manipulating the delicate, friable vessels inside the human cranium carries an inherent risk of stroke or localized hemorrhage hovering around 3% to 5% even in the most elite hands. You are essentially trading a low, continuous annual risk for a sharp, immediate spike of procedural risk on a Tuesday morning in an operating room.
Common mistakes and misconceptions
The ticking time bomb myth
Many patients visualize their diagnosis as an active explosive device waiting to detonate during a sneeze. Let's be clear: this mental image destroys your quality of life unnecessarily. Medical registries demonstrate that a staggering 80% to 90% of small vascular anomalies never rupture during a patient's natural lifespan. Why do we assume every bulge is a death sentence? The problem is that human brains struggle with probability. You read a tragic headline, and suddenly your 3-millimeter incidental finding feels like a lethal threat. It is not.
Assuming size is the only risk factor
Big means bad, right? Except that reality refuses to be so accommodatingly simple. While a larger diameter increases danger, morphology and location dictate true fragility with vicious unpredictability. A small, irregular, multi-lobulated outpouching on the posterior communicating artery can pose a far greater threat than a smooth, larger sac elsewhere. Doctors evaluate the aspect ratio and hemodynamic stress. But patients frequently obsess over millimeters alone, which explains why so many seek unnecessary, high-risk interventions for stable anomalies.
The hemodynamic blind spot and expert advice
What your doctor isn't telling you about inflammation
Can you live with an unruptured brain aneurysm without addressing your systemic biology? Hardly. Most clinical conversations focus heavily on surgical clipping or endovascular coiling. Yet, the invisible culprit driving structural degradation is vascular wall inflammation. Endothelial dysfunction acts as the silent accomplice. Academic research indicates that active matrix metalloproteinases degrade the collagen matrix within the vessel wall. As a result: local shear stress transforms a stable bulge into a vulnerable one. This is why strict blood pressure management and immediate tobacco cessation are mandatory. Smoking increases the risk of growth and eventual rupture by an astonishing factor of three to four, rendering lifestyle modifications just as vital as a neurosurgeon's tools. (We must acknowledge that modern imaging cannot perfectly predict wall tensile strength, forcing us to rely on these surrogate lifestyle markers.)
Frequently Asked Questions
What are the actual annual statistics for a rupture?
The annual risk of a rupture for a small, asymptomatic vascular sac measuring under 7 millimeters in the anterior circulation is roughly 0.1% per year. This translates to a 1 in 1000 chance annually, a figure that surprises most terrified patients. Conversely, giant lesions exceeding 25 millimeters carry an alarming five-year rupture rate of approximately 40%. These numbers fluctuate wildly based on your specific medical history, geographic location, and familial background. Neurologists utilize these stratified metrics from the International Study of Unruptured Intracranial Aneurysms to determine if the danger of brain surgery outweighs the danger of observation.
Can I safely exercise with an unruptured brain aneurysm?
Yes, but you must completely banish intense isometric straining, heavy powerlifting, and violent breath-holding techniques. Moderate cardiovascular activity like brisk walking, cycling, and swimming actually optimizes endothelial health and reduces systemic vascular resistance. The issue remains that sudden, massive spikes in intracranial pressure can exert dangerous mechanical stress on fragile arterial walls. Can you live with an unruptured brain aneurysm while maintaining an active lifestyle? Absolutely, provided you substitute extreme exertion with controlled, aerobic movement that keeps your heart rate within a predictable, doctor-approved zone.
Does emotional stress cause immediate rupture?
Chronic psychological distress erodes your vascular lining over time through sustained cortisol elevation, but a sudden argument rarely triggers an immediate catastrophic event. Acute, explosive rage has been linked to transient blood pressure surges that could theoretically push a highly unstable, critical lesion over the edge. However, daily anxieties about your diagnosis are far more damaging to your mental health than they are to your intracranial arteries. Seeking psychological support to process the diagnosis is a vital, frequently overlooked component of conservative medical management.
A definitive medical stance on your diagnosis
An unruptured cerebral bulge should be treated as a chronic vascular condition requiring vigilant management rather than an immediate surgical emergency. We must stop rushing terrified patients onto the operating table when conservative surveillance is objectively safer. Modern endovascular tools are marvels of human ingenuity, but they carry inherent risks of stroke and neurological deficit that frequently eclipse the natural history of the condition. True medical wisdom lies in knowing when to leave